

Clinical diagnosis
Case 15
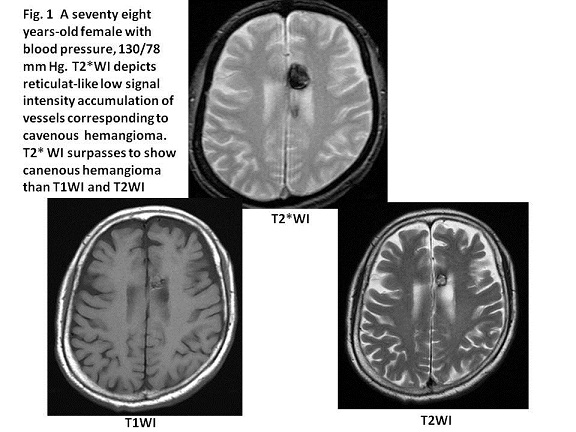
The most common type of cavernous hemangioma owns a“popcorn ball”configuration: a well-margined complex and reticulated core of mixed signal intensity on T1 weighted image (WI) and T2WI due to the hemorrhage of the various stages (1). Multiple lesions at different locations are seen in approximately a half of patients with cavernous hemangiomas (1). Figure 1 is the case whose configuration of T2*WI has the accumulation of hypo-signal reticulated component, and both images of T1WI and T2WI have the mixed signal intensity.
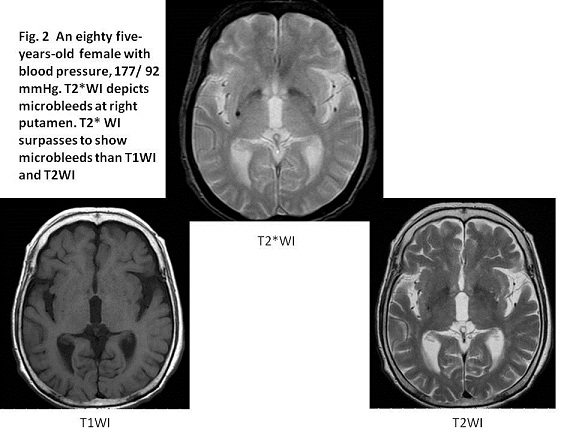
T2*WI is being included for MRI brain dock because T2*WI has the high sensitivity to detect cerebral microbleeds (CMBs). The incidences of CMBs are 7 % in community-dwelling healthy residents of 45 to 50 years-old and 36 % in those of 80 years-old or older in Rotterdam group (2), and 6 % in those of 60 years-old or older in Japan (3). Meanwhile, the incidence of CMBs is 21-78 % and 47-80 % in the patients with brain infarction and those with brain hemorrhage (4). The presence of CMBs is inferred the highly risk factor for occurring brain hemorrhage. Because the prospective study of between CMBs and the first onset of intracerebral hemorrhage revealed that CMBs were detected in 69 % of the group with brain hemorrhage, while in 27 % of the control group (5), it is concluded that the presence of CMBs is the independent risk factor for the first onset of intracerebral hemorrhage (5). Figure 2 is the brain dock case of the hypertensive microbleed at the basal ganglion. The preventive anti-hypertension agent might be given for this patient.
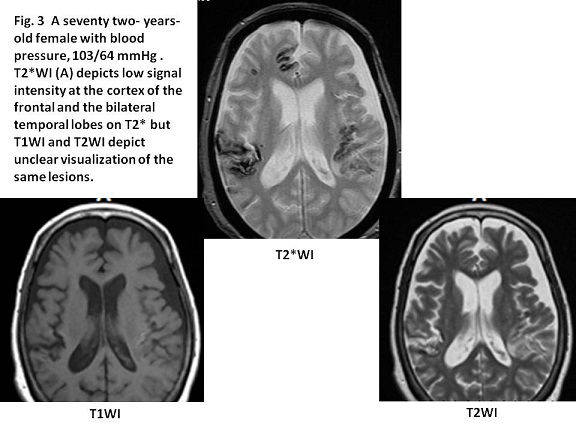
Meanwhile, CMBs at the cortex or sub-cortex white matter are involved with amyloid angiopathy (6), which is caused by the deposition of beta-amyloid in the arterial media and/or adventitia of small arteries and arterioles in the meninges and cortex. In elderly patients, lobar intracranial hemorrhage and multiple microbleeds are highly suggestive of CAA (6). Figure 3 is the same as Case 14 in the series of “Case of the week” which showed the cortex bleeding.
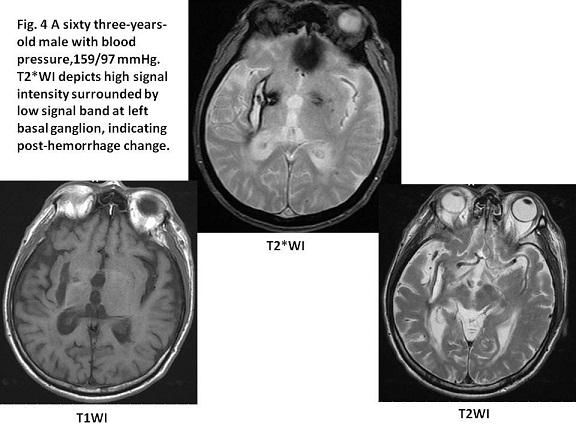
Hypertensive brain hemorrhage is known to be caused by the rupture of the lenticulostriate arterial branches of the middle cerebral artery, leading to putaminal or caudate hemorrhage and the small perforating branches, leading to pontine or thalamic bleeds (7). Microscopically, fibrinoid necrosis of the ruptured arterial wall is usually found (7). Figure 4 is the typical case of hypertensive intracranial hemorrhage.
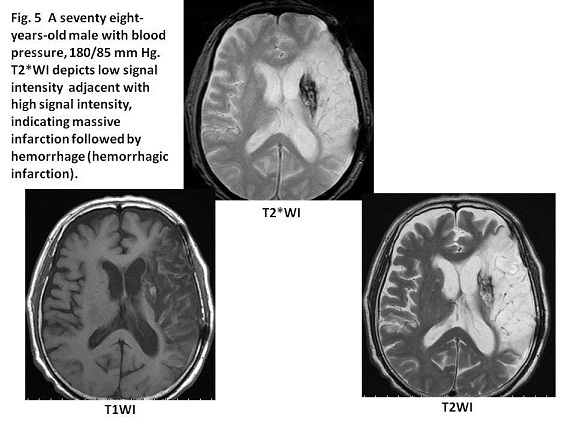
Intra-cerebral hemorrhage sometimes occurs followed by brain infarction. The frequency of the secondary intra-cerebral hemorrhage is not precisely known. The secondary intra-cranial hemorrhage is considered to result from the reperfusion of the necrotic brain tissue caused by the re-canalization of the occluded vessel (7). Figure 5 is the case whose secondary intra-cranial hemorrhage occurred approximately 2 weeks after the first brain stroke.
When hemorrhage occurs, oxyhemoglobin turns into deoxyhemoglobin, methohemoglobin and hemosiderin as time progress. Deoxyhemoglobin, methohemoglobin and hemosiderin are paramagnetic (8), which are found as low signal intensity on T2*WI. As the drawback of T2*WI, it is hard to differentiate new hemorrhage from old hemorrhage because both of deoxyhemoglobin and hemosiderin are visualize low signal intensity in T2*WI.
【Summary】
T2*WI is more sensitive than the other sequence of MRI and CT to detect CMBs. The use of standard MRI without T2*WI sequences increases the potential for overlooking lesions. Although it is hard to infer the age of hemorrhage, T2*WI is useful to identify the cranial micro-bleeds, and might be able to approach to imaging diagnosis with consideration of the bleeding site, hemorrhage configuration, the patient age, the presence or absence of hypertension.
【References】
1.Zabramski JM, et-al. The natural history of familial cavernous malformations: results of an ongoing study. J. Neurosurg.1994;80:422-432. doi:10.3171/jns.1994.80.3.0422 - Pubmed citation
2.Poels MM, et al. Prevalence and risk factors of cerebral microbleeds: an update of the Ritterdam scan study. Stroke 2010; 41: 103-106.
3.Takashima Y, et al. Clinical correlating factors and cognitive function in community-dwelling healthy subjects with cerebral microbleeds, J Stroke Cerebrovasc Dis 2011; 20: 105-110.
4.Koennecke HC. Cerebral microbleeds on MRI: prevalence, associations, and potential clinical implications. Neurology 2006; 66: 165-171.
5.Sun S, et al. Association between cerebral microbleeds and the first onset of intracranial hemorrhage – a 3.0 T MR study. Acta Radiol 2012; 53: 203-207.
6.Sakaguchi,H, et al. Cerebral amyloid angiopathy-related inflammation presenting with steroid-responsive higher brain dysfunction: case report and review of the literature. J Neuroinflammation 2011; 8: 116
7.Atlas SW, Thulborn KR. Intracranial hemorrhage. Magnetic Resonance Imaging of the Brain and Spine. 3rd ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2002. 773-832.
8.Tang MY, et al. Review Article GRE T2-Weighted MRI: Principles and Clinical Applications. BioMed Research International Volume 2014 : Article ID 312142, 12 pages http://dx.doi.org/10.1155/2014/312142
2016.7.20
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.