

Clinical diagnosis
Case 19
As inflammatory deta of CRP and WBC counts were not found, laparoscopic cholecystectomy was first attempted, but not achieved. Laparotomic cholecystectomy was eventually followed. The swollen gallbladder was removed, inducing the improvement of liver function. The patient discharged without complication and was scheduled to get the follow-up examination.
【Discussion】
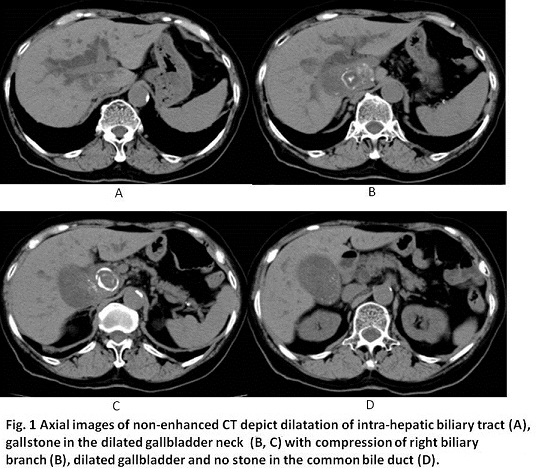
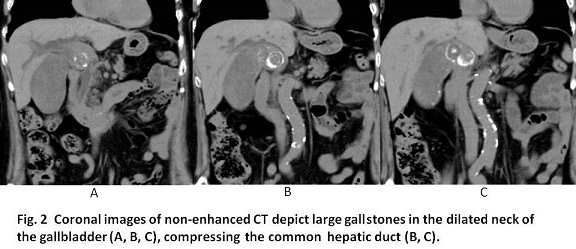
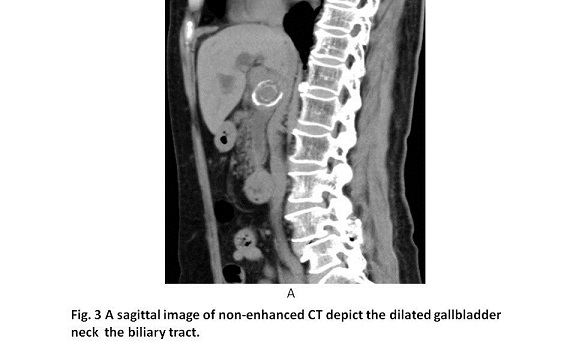
Gallstone alone usually does not cause obstructive jaundice. However, the obstructive jaundice occurs when the edema of gallbladder wall surrounding the gallstone compress the common bile duct whose patho-physiological condition is called Merizzi syndrome (1). Merizzi syndrome occurs secondary to a single large gallstone or multiple small gallstones impacted in the Hartmann’s pouch or in the gallbladder infundibulum (neck) and cystic duct (1-3). In our case, Mirizzi syndrome occurred with a large stone in the gallbladder neck (or cystic duct).
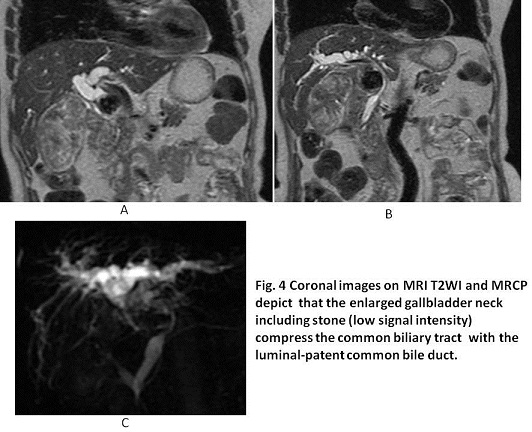
Mirizzi syndrome is largely classified into two types; Type1, in a case for the swollen gallbladder to compress the common bile duct externally without fistula between gallbladder and common bile duct: Type II in a case with fistula between them (1-3). Csendes proposed the classical Type II into new Types II, III, IV and Va, Vb (1). Namely, the new Type II consists of a cholecystobiliary fistula resulting from erosion of the bile duct wall by a gallstone, the fistula must involve less than one-third of the circumference of the bile duct. Type III consists of a cholecystobiliary fistula involving up to two-thirds of the bile duct circumference. Type IV is a cholecystobiliary fistula with complete destruction of the bile duct wall with the gallbladder completely fused to the bile duct forming a single structure with no recognizable dissection planes between both biliary tree structures. Type Va includes a cholecystoenteric fistula without gallstone ileus and Type Vb refers to a cholecystoenteric fistula complicated by gallstone ileus (1). Our case with common bile duct stenosis occurred with the external compression by the swollen gallbladder neck including large stone without any fistula and then, belonged to Mirizzi syndrome Type I.
CT, MRI and magnetic resonance cholangiopancreatography (MRCP) are useful tools to evaluate gallstones, bile duct dilatation, gallbladder wall thickness, extrinsic compression of the bile duct. Especially, MRCP might be favorable to detect the presence or absence of the fistula (1). Kumar et al. reported that of the 169 MS patients were surgically managed between 1989 and 2011, preoperative diagnosis of MS was possible in only one-third of patients in their series (3). In our case, of the three dimensional images, coronal images of CT and MRI were determinant to show the extrinsic compression to the common bile duct and to find no malignancy, and coronal images of MRCP showed no evidence of fistulas between gallbladder and common bile duct and between gallbladder and intestinal bowels, leading to diagnosis of Merizzi syndrome Type I.
Laparoscopic cholecystectomy is prevailing worldwide but in case of Mirizzi syndrome, it can be dangerous for the bile duct injury (1, 3). Some conditions such as the difficult identification of the cystic duct and the unpredictable fistula increase the risk of bile leakage in laparoscopic cholecystectomy (1). In our case, classical cholecystectomy was eventually conducted under open surgery.
【Summary】
We present a seventy six-year-old female with Merizzi syndrome Type 1 which a swollen gallbladder neck including a impacted large stone compressed the common bile duct causing elevation of total bilirubin and liver dysfunction. Coronal images of CT, MRI and MRCP were useful to recognize the relation of swollen gallbladder neck with the compression of the common bile duct. The patient received a total cholecystectomy without any complication, instead of laparoscopic chlecystectomy. Mirizzi syndrome progress Type I to Vb, the more delayed diagnosis induces the more difficult surgical management because of the presence of the fistula between gallbladder and common bile duct or enteric bowel. The early diagnosis prior the fistula formation and the decent surgical treatment brought about the speedy recovery in our case
【References】
1.Beltran MA. Mirizzi syndrome: History, current knowledge and proposal of a simplified classification World J Gastroenterol. 2012; 18: 4639-4650 Published online Sep 14, 2012. doi: 10.3748/WJG.v18.i34.4639
2.Petricevic PB Mirizzi syndrome--two case reports and a short review of the literature.Int Surg. 2011;96:228-232.
3.Kumar A, et al. Mirizzi's syndrome: lessons learnt from 169 patients at a single center. Korean J Hepatobiliary Pancreat Surg. 2016;20:17-22. doi: 10.14701/kjhbps.2016.20.1.17. Epub 2016 Feb 19.
2016.8.17
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.