

Clinical diagnosis
Case 20

Although he did not receive liver biopsy, the routine bone marrow puncture prior to chemotherapy was conducted for confirming the presence or absence of healthy bone marrow. It revealed malignant cells by accident, yielding to diagnosis of diffuse large B cell lymphoma, indicating Stage IV malignant lymphoma
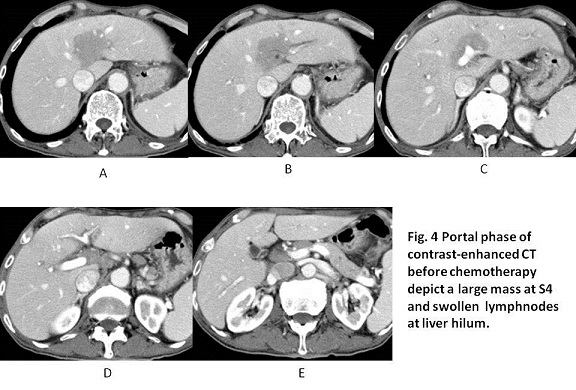
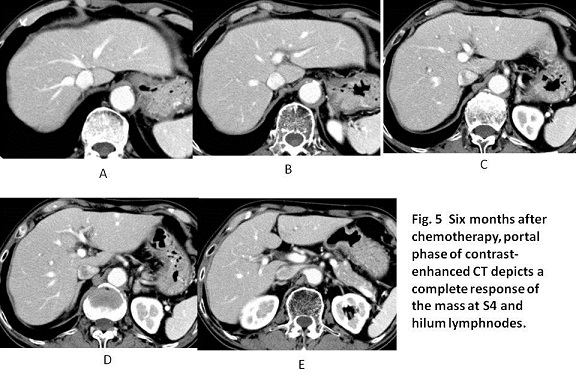
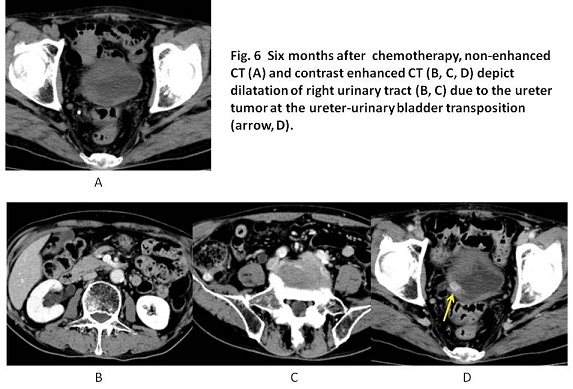
Six months after he had four courses of R-THP-COP chemotherapy, he received contrast-enhanced CT which showed the complete response of tumor disappearance. (Figs 4, 5). However, at the same time, ureter tumor at the outlet of the ureter was visualized (Fig. 6 B, C, D). Thereafter, he underwent surgical resection of the lower part of the ureter and vescico-ureter anastomosis. Pathological examination revealed transitional cell carcinoma. He is scheduled routinely to come to our hospital every 3 months for the follow-up examination.
【Discussion】
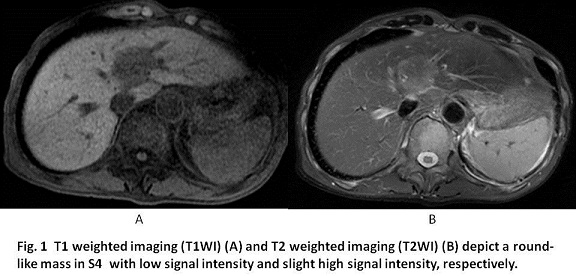
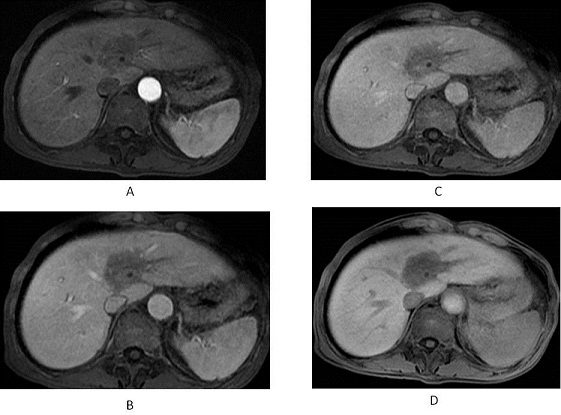
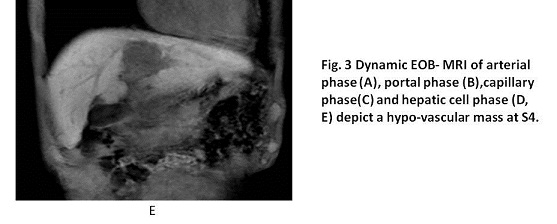
Hepatic lymphoma does not encounter so often. The image findings of CT and MRI of the hepatic lymphoma either primary or secondary, are known to be non-specific such as homogeneous hypodense with clear margin on CT, low and high signal intensity on TI- and T2-weighted MR (1, 2). Dong A, et al. recently reported a case of the hepatic mucosa-associated lymphoid tissue (MALT) whose image showed the vessels and bile ducts had no distortion or displacement (3). In our case of diffuse large B cell lymphoma, EOB enhanced MRI depict a hypovascular mass with clear margin was growing with no displacement or invasion of portal vein and bile duct but it invaded along with Glisson sheath (probably lymphatic channel). Hepatic malignant lymphoma might be taken into consideration when a hepatic mass have minimal mass effect with portal veins and bile ducts normally passing through the tumors.
Hepatitis C virus or hepatitis B virus (HBV) infection was reported to be more prevalent in malignant lymphoma (4, 5, 6). Taborelli M, et al reported that HCV infection was detected in 11.1 % of non-Hodgikin lymphoma (NHL) cases and 3.5 % of cohort controls, while HBV infection was detected in 3.7 % of NHL cases vs 1.7 % of cohort controls in Italy (5). Of the autoimmune disease, Sjögren's syndrome is known to be the highest incidence of malignant lymphoproliferative disorders transformation (6). Our case had the occult infection of HVB. Although he had no history of Sjögren's syndrome, ureter cancer was followed to occur six months later after the initial onset of malignant lymphoma.
The standard chemotherapy of Stage IV NHL involves chemotherapy, frequently a regimen called R-CHOP. R-CHOP stands for the chemotherapy drugs cyclophosphamide, doxorubicin, vincristine, and prednisone, with the addition of rituximab, a monoclonal antibody. Lymphoma treatments continue to improve. The five-year relative survival rate climbed to 61 to 82 percent (2001-2007) (7, 8). The average survival time of NHL patients with monocytes (%) ≥ 8% was reported to be shorter than those with monocytes (%) < 8% (8) Our case with monocytes of 15.6% received four courses chemotherapy of R-THP-COP, resulting in complete response of the hepatic lymphoma. However, the further follow-up is necessary for the better outcome.
【Summary】
We present a case with the hepatic lymphoma (diffuse large B cell lymphoma) whose images of EOB enhanced MRI and contrast-enhanced CT revealed a hypovascular mass with clear margin and with portal veins and bile ducts normally passing through the tumors. Further, the tumor involved in the Glisson sheath and hepatic hilum lymphnodes. Although the latest chemotherapy was effective for the complete response of malignant lymphoma, the ureter cancer occurred six months later. The patient also had the occult HBV infection. We should keep in mind that the typical image of the hepatic lymphoma and its relevant underlying disease, and the possible occurrence of other malignancy.
【References】
1.Gazelle GS, et al. US, CT, and MRI of primary and secondary liver lymphoma. J Comput Assist Tomogr. 1994;18: 412-415.
2.Khaled M, et al. Focal Hepatic Lesions: Diagnostic Value of Enhancement Pattern Approach with Contrast-enhanced 3D Gradient-Echo MR Imaging. RadioGraphics. 2005; 25:1299-1320
3.Dong A et al. CT, MRI, and 18F-FDG PET/CT Findings in Untreated Pulmonary and Hepatic B-Cell Lymphoma of Mucosa-Associated Lymphoid Tissue (MALT) Over a Five-Year Period: A Case Report. Medicine (Baltimore). 2016 Mar;95(12):e3197. doi: 10.1097/MD.0000000000003197.
4.Tajima K High prevalence of diffuse large B-cell lymphoma in occult hepatitis B virus-infected patients in the Tohoku district in Eastern Japan. J Med Virol. 2016 May 24. doi: 10.1002/jmv.24584. [Epub ahead of print]
5.Taborelli M, et al. Hepatitis B and C viruses and risk of non-Hodgkin lymphoma: a case-control study in Italy. Infect Agent Cancer. 2016 Jun 23;11:27. doi: 10.1186/s13027-016-0073-x. eCollection 2016.
6.Gorodetskiy V, et al. Primary Diffuse Large B-Cell Lymphoma of the Liver in a Patient with Sjogren Syndrome. Case Rep Oncol Med. 2016;2016:2053257. doi: 10.1155/2016/2053257. Epub 2016 Feb 22.
7.Stephens DM, et al. Continued Risk of Relapse Independent of Treatment Modality in Limited-Stage Diffuse Large B-CellLymphoma: Final and Long-Term Analysis of Southwest Oncology Group Study S8736. J Clin Oncol. 2016 Jul 5. pii: JCO654582. [Epub ahead of print]
8.Wu C, et al. Prognostic Significance of Monocytes and Monocytic Myeloid-Derived Suppressor Cells in Diffuse Large B-Cell Lymphoma Treated with R-CHOP. Cell Physiol Biochem. 2016 Jul 7;39(2):521-530. [Epub ahead of print]
2016.8.24
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.