

Clinical diagnosis
Case 23
Her symptoms were getting improved. Contrast-enhanced CT depicted no ischemia of the digestive bowels because blood flow of false lumen reentered to true lumen of peripheral SMA branches. The follow-up contrast-enhanced CT 2 months and 5 months later showed no expansion of SMA dissection. She continues to take anti-hypertension agents.
【Discussion】
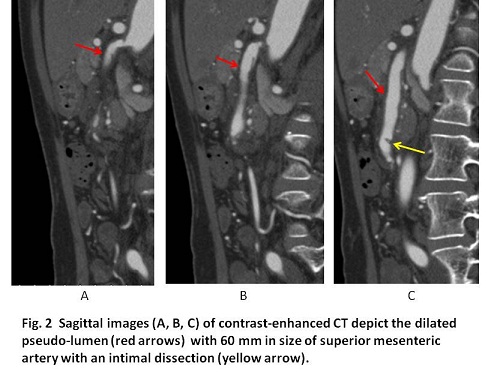
Superior mesenteric arterial (SMA) dissection occurs as part of aortic dissection or on its own isolated. The isolated SMA dissection was rare but the most frequently reported type of visceral artery dissection (1-5). It usually begins at a few centimeters from the SMA origin (1-5). Splis et al proposed the hypothesis that the isolated SMA dissection was caused by the stress on the wall of the artery on the inferior pancreatic edge (2, 3). Although atherosclerosis, fibrodysplasia, connective tissue disorders, and trauma were listed (1-5), the definite etiology of the isolated SMA dissection was not known. Patients often present in middle age (3). The age of our case was fifty five years old. Our case had a history of hypertension. The dissection (pseudo-lumen) of 6 cm long distance occurred from 0.8 cm distal from SMA inlet and entered into to the true lumen. A few jejunum branches and pancreatic branches occluded but no ischemic changes of the bowel and pancreas were found in contrast-enhanced CT probably owing to the blood supply from the distal anastomosis of the peripheral SMA branches and pancreatic arterial arcades.
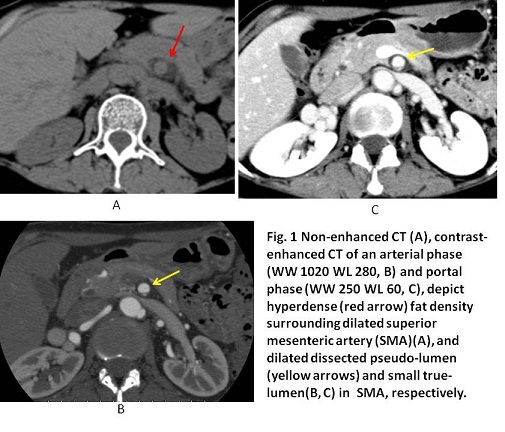
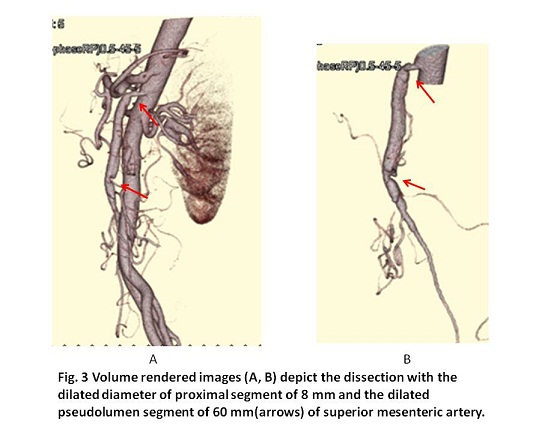
As the typical images of SMA dissection, it is reported that on non-enhanced CT, the SMA is often enlarged and there can be increased attenuation of the fat around the SMA in an acute state, and on contrast-enhanced CT, the dissected intimal flap is often found out (4). In our case, non-enhanced CT showed the enlarged SMA with slight hyperdense fat surrounding the SMA and contrast enhanced CT showed the true and false lumens and no ischemic change of the bowels. The maximum intensity projection (MIP) image and 3DCT reconstruction volume rendered (VR) image were useful to identify the extent of the dissection.
Different treatment choices are possible for SMA dissection ranging from watchful observation to surgical revascularization or to endovascular therapy (1-6). The optimal therapy for isolated SMA dissection depends on the patient situation and remains controversial. In cases of hemorrhagic or expanding SMA pseudoaneurysm or ischemic bowels, invasive treatments are necessary (6). In these days, the reports of endovascular therapy are increasing (1, 3, 5, 6). The prognosis is variable and it can sometimes be fatal (1-6). In our case, the invasive treatment was unnecessary since the symptoms were getting improved and no bowel ischemia was found. Six months later, the follow-up contrast-enhanced CT, showed no expansion of the dissected SMA.
【Summary】
We present a fifty five-year-old female with SMA dissection, whose symptoms were back pain and epigastric pain. Non-enhanced CT showed the enlarged SMA with slight hyperdense fat surrounding the SMA and contrast enhanced CT showed the 6 cm-long pseudo-lumen with almost collapsed false lumen and well-enhanced bowel. She made a choice of conservative management because of her symptoms getting improved. The follow-up CT six months later showed no expansion of the dissected SMA.
【References】
1.Gobble RM, Brill ER, Rockman CB et-al. Endovascular treatment of spontaneous dissections of the superior mesenteric artery. J. Vasc. Surg. 2009;50 (6): 1326-32.
2.Hirai S, Hamanaka Y, Mitsui N, Isaka M, Kobayashi T. Spontaneous and isolated dissection of main trunk of the superior mesenteric artery. Ann Thorac Cardiovasc Surg 2002;8:236-40.
3.Solis MM, Ranval TJ, McFarland DR, Eidt JF. Surgical treatment of superior mesenteric artery dissecting aneurysm and simultaneous celiac artery compression. Ann Vasc Surg 1993; 7: 457–62
4.Suzuki S, Furui S, Kohtake H et-al. Isolated dissection of the superior mesenteric artery: CT findings in six cases. Abdom Imaging. 29 (2): 153-7.doi:10.1007/s00261-003-0110-2 - Pubmed citation
5.Min SI, et al. Current strategy for the treatment of symptomatic spontaneous isolated dissection of superior mesenteric artery. J Vasc Surg. 2011;54:461-466. doi: 10.1016/j.jvs.2011.03.001. Epub 2011 May 14.
6.Nakai, et al. Endovascular stenting and stent-graft repair of a hemorrhagic superior mesenteric artery pseudoaneurysm and dissection associated with pancreaticoduodenectomy. J Vasc Interv Raiol 2012; 23: 1381-1384
2016.9.14
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.