

Clinical diagnosis
Case 24
The reference doctor at the local hospital where the patient had received drip infusion last night called us that his blood culture revealed pneumococcus infection (Streptococcus pneumonia). He recommended us to prescribe antibiotics of Sulbactam/Ampicillinfor for the bacteria. We already used them from the beginning. Despite them, the patient condition rapidly worsened and soon after, a lot of petit hemorrhagic spots were found in his lower extremities. Laboratory test 10 hours after admission revealed hyperkalemia (7.7mEq/L). Hemodialysis was hesitated to conduct because of the situation of hemorrhagic tendency. Regrettably, he passed away because of cardiac arrest.
【Discussion】
The serious heat stroke symptom usually appears with a core body temperature of 40 °C or higher. The first sign might be fainting (1). According to the guideline of heat stroke (2), three grades are proposed; Grade 1 dizziness, faint and lack of sweating usually called sunstroke; Grade II heat malaise, headache and vomit; Grade III symptoms of central nerve system disorder of convulsion, seizure and unconsciousness, visceral organ disorder and/or coagulopathy. Our body is usually able to disperse the heat through skin or by sweating. However, in extreme heat, high humidity or vigorous physical exertion, the body may be unable to accommodate the body temperature (1). Further, dehydration is another cause of heat stroke (1, 2). In our case, the patient worked under the sun for a long time and got diarrhea all day. He was diagnosed Grade II heat stroke in a local hospital at last night of Day 1.
Pneumococcus is gram-positive bacteria formally named streptococcus pneumonia microscopically covered with thick capsule (3). Pneumococcus is one of the common bacteria easy to adhere to nasal and throat membrane. As pneumococcus diseases, pneumonia is the most common. The other parts of the body are infected such as middle ear, sinus and meninges causing pneumococcal otitis media, sinusitis and meningitis, respectively (3, 4). On the other hand, pneumococcus is known to cause extremely fulminate infection (5-9). Bacteremia or sepsis is a type of invasive pneumococcal disease that infects the blood (5). It occurs in patients with immune disorder such as post-splenectomy, collagen disease, HIV infection, diabetes mellitus, multiple myeloma (5). Our patient was a healthy adult but he worked outside for more than 10 hours under hot summer sky. He got heat stroke resulting from prolonged exposure to high temperatures, inducing immune disorder and resulting in the invasive pneumococcal bacteremia.
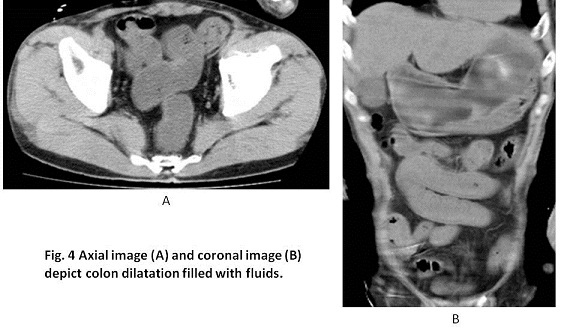
There are few reported cases of enteritis caused by pnumococcus in the previous literature (8). Because our patient had no other apparent inflammation site, we believe he got pneumococcal enteritis with bacteremia.
Toxin from bacteremia induces to release of cytokine from systemic body cells in order to eliminate bacteria in blood, inducing septic symptoms. In short, cytokine release incurs various adverse effects such as hypotension of blood pressure due to vessel dilatation and intravascular coagulation of capillaries in systemic organs (10). As a result, the decreased blood flow of life-preserving organ such as kidney, heart and brain, make heart activity aggressively with rapid cardiac beat and increased cardiac output which sooner or later, leads to weaken the cardiac function and to reduce the blood flow to the life-preserving organs (10). The negative cycle rotates; dysfunction of kidneys; accumulation of lactic acids and K in blood; oozing out of serum from pulmonary vessel to pulmonary air space: poor ventilation of lung inducing severe dyspnea (10). This situation is called multiple organ failure which is caused by sepsis with DIC. Our patient was a healthy adult and got an invasive pneumococcal infection as a trigger of heat stroke. Although invasive pneumococcal infection was known to occur in healthy adult (8, 9, 11), heat stroke was least known to worsen the symptoms of pneumococcal infection. Eventually, the lower limbs of our patient showed rapidly progressive purpura of petit hemorrhage, implying to fall in DIC.
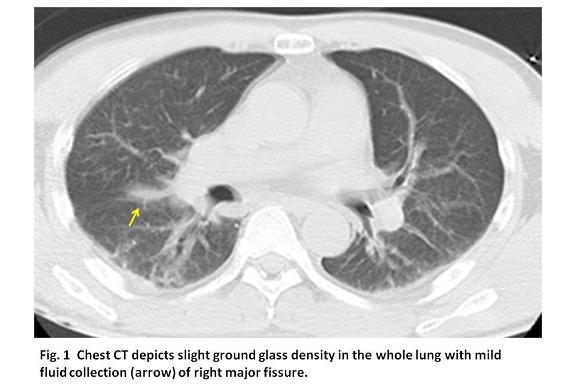
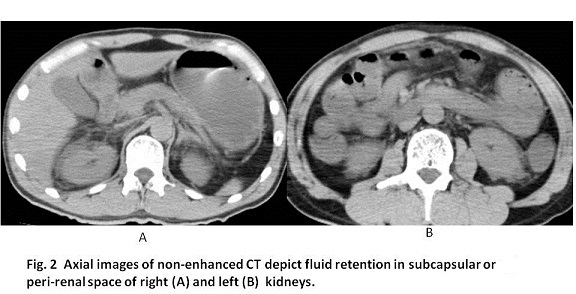
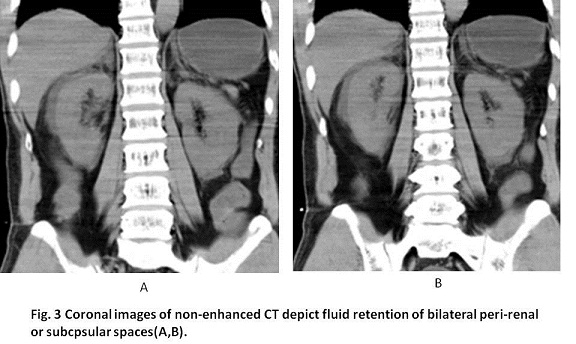
Further, in our case, non-enhanced CT showed homogeneous slight high density in the lung and sub-capsular fluid of bilateral kidneys. We believe that these findings resulted from the oozing of body fluids, which was caused by vessel dilatation and intravascular coagulation of capillaries by sepsis with DIC.
【Summary】
We present a forty seven-year-old male with rapidly progressive fatal pneumococcal sepsis. He was basically a healthy adult but he got heat stroke and immune disorder by exposure of high temperature in hot summer which was triggered by pneumococcal infection, bacteremia and enteritis, eventually becoming sepsis with DIC. The risk of heat stroke accompanied with pneumococcal infection was yet to be known. Non-enhanced CT showed homogeneous slight high density in the lung and fluid retention surrounding bilateral kidneys, corresponded to the oozing of body fluids due to DIC. We should keep in mind these findings indicating DIC.
【References】
1.Anthony F, et al. 2008: Harrison's Principles of Internal Medicine (17th ed.). McGraw-Hill Professional. pp. 117–121. ISBN 978-0-07-146633-2.
2.Miyake Y, et al. 2015: Guideline of heat stroke. (in Japanese)
3.Kalin M, et al. Prospective study of prognostic factors in community-acquired bacteremia pneumococcal disease in 5 countries. J Infect Dis 2000; 182: 840-847
4.Musher DM, et al. Bacteremic and nonbacteremic pneumococcal pneumonia: a prospective study. Medicine 2000; 79: 210-221
5.Taylor SN, et al. Unusual manifestation of invasive pneumococcal infection. Am J Med 1999; 107: 12-27
6.Carpenter CT, et al. Purpura fulminans in pneumococcal sepsis: case report and review. Scand J Infect Dis 1997; 29: 479-483
7.Murph RC, et al. Rapid fatal oneumococcal sepsis in a healthy adult. Clin Infect Dis 1996; 22: 375-376
8.Soman RN, et al. Acute enteritis associated with pneumococcal bacteremia. J Assoc Physicians India. 2009; 57: 173-174
9.Takada K, et al. Purpura fulminans due to pneumococcal pneumonia in a healthy adult. JJA. Inf. D. 2007; 81: 194-199 (Japanese)
10.Levi M et al. Disseminated intravascular coagulation: What's new? Crit Care Clin. 2005; 21: 449-67.
11.Iinuma Y, et al. Rapidly progressive fatal pneumococcal sepsis in adults: a report of two cases. J Infect Chemother. 2007; 13: 346-349.
2016.9.21
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.