

Clinical diagnosis
Case 46
After surgical management, all patients discharged without any complication.
【Discussion】
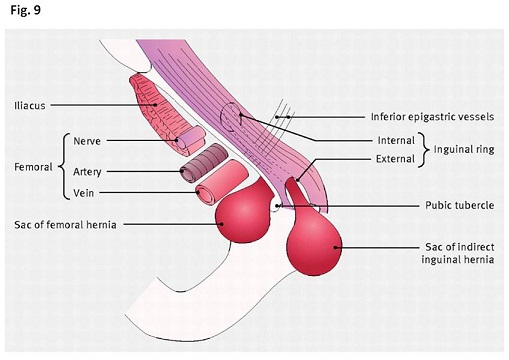
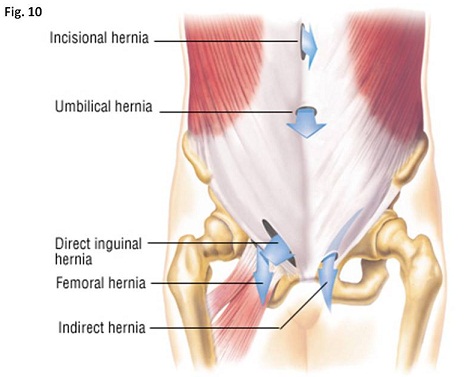
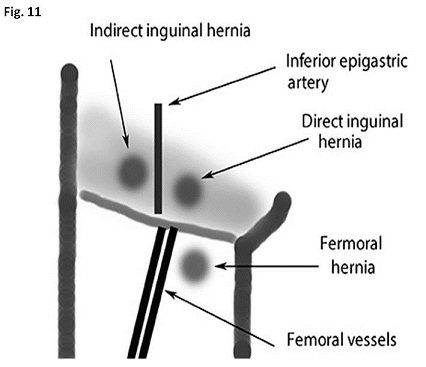
There exist three hernias at the groin lesion: indirect inguinal hernia, direct inguinal hernia and femoral hernia. Indirect inguinal hernia happens indirectly via the inguinal canal and direct hernia protrudes directly via the weak portion of the abdominal muscle. Femoral hernia comes out from the femoral canal which is present at the medial side of the femoral vein(Fig.9-11).
The closure of the abdominal cavity finalize by lining and extending of the transverse fascia to the inguinal canal. In males, the closure of the inguinal canal happens a few weeks before or after since the spermatic cord and testis descend from the inside of the abdomen to the scrotum via the route of the inguinal canal. Meanwhile, in females, the closure of the inguinal canal finalize occurs a couple of months before birth since the ovary does not descend out of the abdominal cavity. Further, in females, the round ligaments pass through the inguinal canal and support the uterus, inducing the additional cover with the abdominal cavity. Hence, the inguinal hernia happens less in female than male.
The lifetime risk of abdominal hernia is reported 5 % of general population. Eighty percent of the abdominal hernia is inguinal hernia and 5 percent, femoral hernia (1-4). The other report says that approximately 25 % of males and approximately 2 % of females will experience groin hernia in their life time (5). Indirect inguinal hernias occur usually in males of babies to young adults with leaving an opening at the upper part of the inguinal. The opening site is usually lateral to the inferior epigastric vessels. Indirect inguinal hernia is the most common type of the groin hernias and known to appear in 2 to 3 % in male children and less than 1 % in female children (5). In females, the ovaries possibly slide into the inguinal canal, inducing hernias. Direct inguinal hernias also usually occur in adults males older than age 40 (1-3). Abdominal wall weakness due to age, stress or strain induces the hernia around the inguinal canal. The opening site is usually medial to the inferior epigastric vessels.
Meanwhile, femoral hernias are more common in females unlike inguinal hernias. The opening site is usually inferior to the inferior epigastric vessels and medial to the common femoral vein. Femoral hernias are reported to occur lateral to the pubic tubercle and compress the femoral vein, which is true in case of localized femoral hernia but not always in case of large femoral hernia.
Groin hernias possibly cause the complications of incarceration and strangulation. Incarceration means the hernia content stuck in the groin area and cannot go back into the abdomen even with the assistance of the manual management. Strangulation means the obstruction of feeding arteries of the herniated content, inducing ischemic necrosis sooner or later. Indirect hernias and direct hernias sometimes can go back into the abdomen with gentle maneuver, while femoral hernias are difficult to go back because inguinal ligaments compress the herniated content from the upper side. In short, the risk of strangulation is lowest for direct inguinal hernia, moderate for indirect inguinal hernia whereas approximately 40 % of femoral hernias develop strangulation.
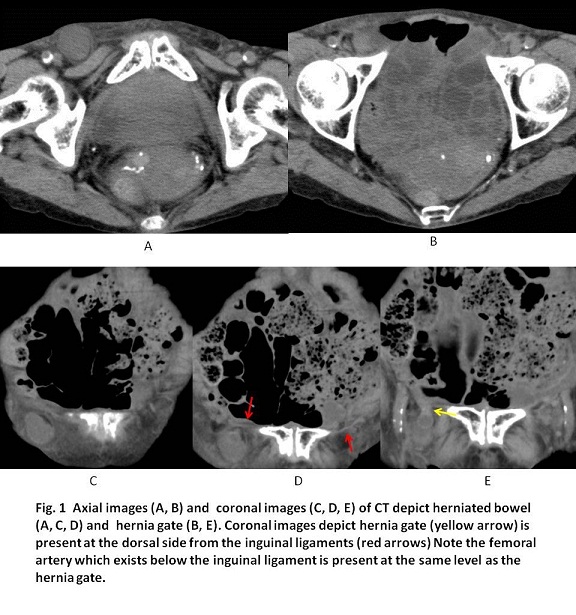
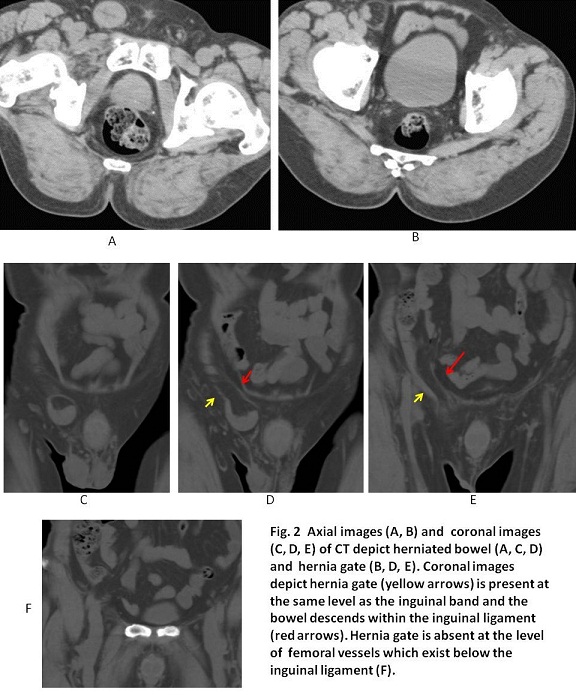
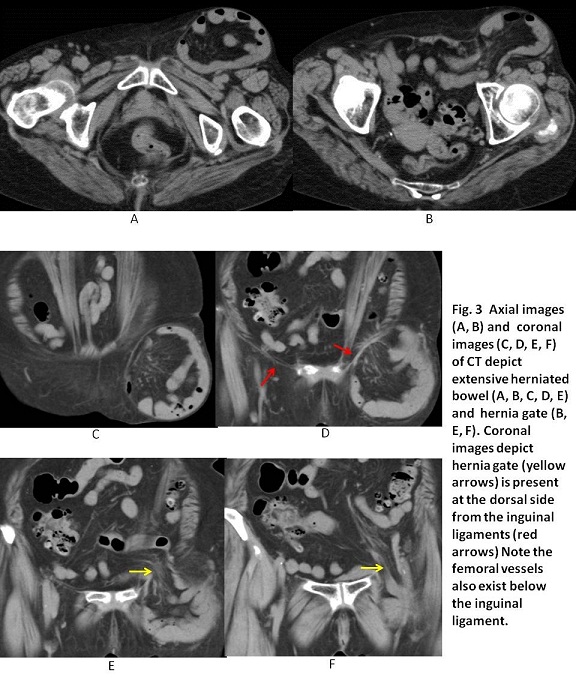
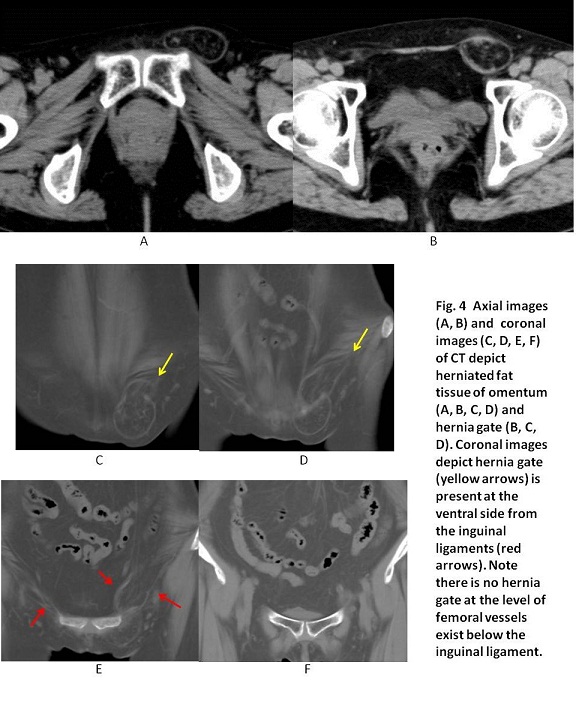
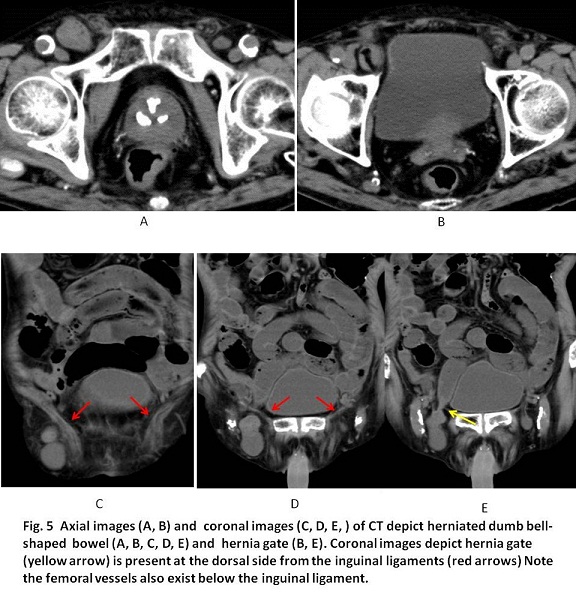
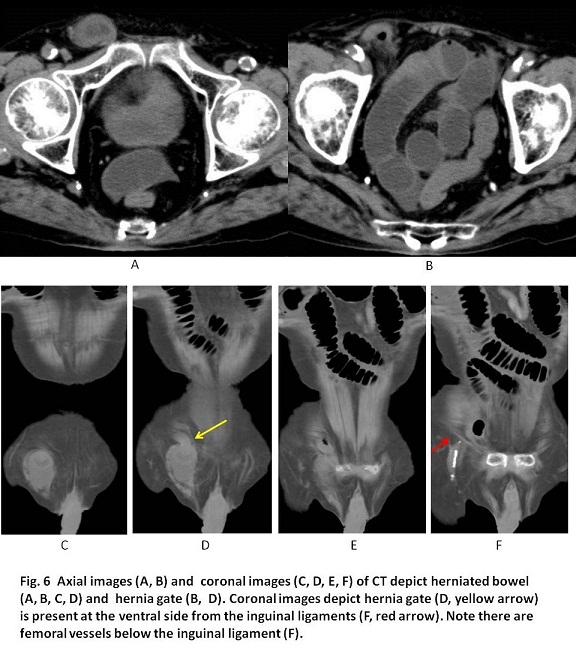
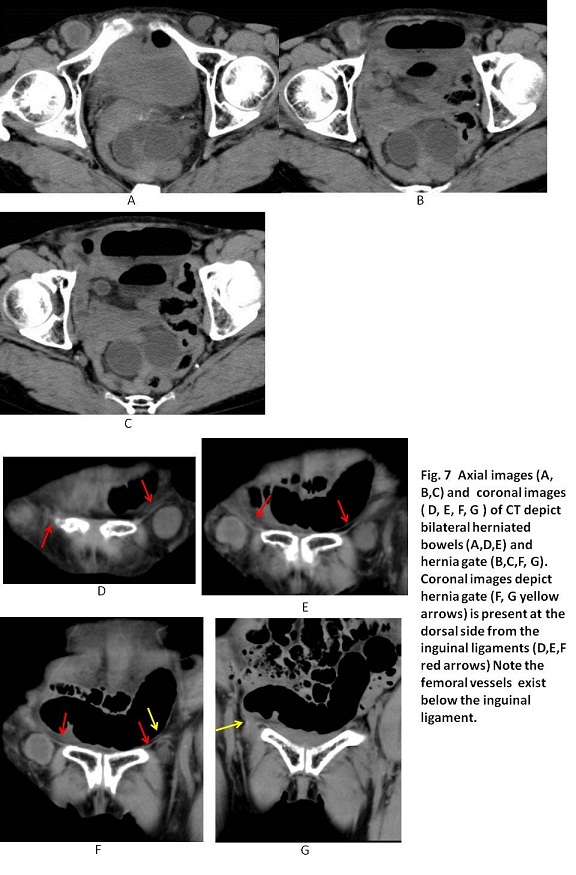
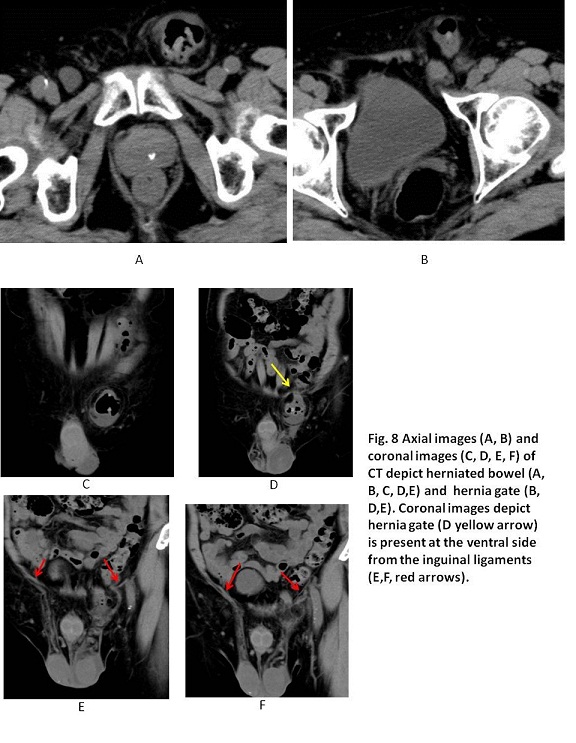
In the previous literature on differentiation between inguinal hernias and femoral hernias, the relations of hernia content with inferior epigastric vessels, a femoral vein and a pubic tubercle were documented using axial images of abdomen CT which were previously thought to be mainstay of the diagnostic tool (3, 5-8). However, the exact differentiation of axial images of non-enhanced CT are difficult to distinct because inferior epigastric vessels are difficult to identify, compression of femoral vein for the characteristic finding for femoral hernia is meaningless for the small femoral hernia, medial site of pubic tubercle for the characteristic finding for indirect inguinal hernia is also meaningless for the large indirect hernia. As explained in figure legends, coronal images of CT are determinant to distinct among indirect inguinal hernia, direct inguinal hernia and femoral hernia. The lower and dorsal edge of inguinal ligament is clearly visualized in coronal CT and the relation of the lower edge with the hernia gate (inlet) is crucial to distinct among them. Namely, the hernia gate is situated at the upper lateral side for indirect inguinal hernia, the gate at the upper medial side for direct inguinal hernia and the gate at the inferior side for femoral hernia. As a result, Figs 2 and 4 were indirect inguinal hernias, Figs 6 and 8, direct inguinal hernias and Figs 1, 3, 5 and 7, femoral hernias.
【Summary】
The lifetime risk of abdominal hernia is reported 5 % of general population. There exist three hernias at the groin lesion: indirect inguinal hernia, direct inguinal hernia and femoral hernia. Of the all abdominal hernias, inguinal hernia occurs in 80 % and femoral hernia in 5 %. Indirect inguinal hernia is the most common type of the groin hernias and known to appear in 2 to 3 % in male children. Direct inguinal hernias also usually occur in adults males older than age 40. Abdominal wall weakness due to age induces the hernia around the inguinal canal. Femoral hernias are more common in females unlike inguinal hernias. Coronal images of CT are determinant to distinct among indirect inguinal hernia, direct inguinal hernia and femoral hernia. The hernia gate is situated at the upper lateral side for indirect inguinal hernia, the gate at the upper medial side for direct inguinal hernia and the gate at the inferior side for femoral hernia.
【References】
1.Greenfield LJ. Review for surgery: scientific principles and practice. Philadelphia, Pa: Lippincott Williams & Wilkins, 2001.
2.Rubenstein RS, Rand Corporation, US Department of Health and Human Services. Surgical conditions. Santa Monica, Calif: Rand, 1983.
3.Suzuki S, Furui S, Okinaga K et-al. Differentiation of femoral versus inguinal hernia: CT findings. AJR Am J Roentgenol. 2007;189 (2): W78-83. doi:10.2214/AJR.07.2085 - Pubmed citation
4.Bailey H, Love RJM, Russell RCG, Williams NS, Bulstrode CJK. Bailey and Love’s short practice of surgery. London, England: Arnold, 2000
5.Whalen HR, Kidd GA, O'Dwyer PJ. Femoral hernias. BMJ. 2011;343 (dec08 1): d7668. BMJ (full text) - doi:10.1136/bmj.d7668 - Pubmed citation
6.Burkhardt JH, Arshanskiy Y, Munson JL et-al. Diagnosis of inguinal region hernias with axial CT: the lateral crescent sign and other key findings. Radiographics. 2011;31 (2): E1-12. Radiographics (full text) - doi:10.1148/rg.312105129 - Pubmed citation
7.Kitami M, Takase K, Tsuboi M et-al. Differentiation of femoral and inguinal hernias on the basis of anteroposterior relationship to the inguinal ligament on multidimensional computed tomography. J Comput Assist Tomogr. 2009;33 (5): 678-81. doi:10.1097/RCT.0b013e3181977a0a - Pubmed citation
8.Cherian PT, Parnell AP. The diagnosis and classification of inguinal and femoral hernia on multisection spiral CT. Clin Radiol. 2008;63 (2): 184-92. doi:10.1016/j.crad.2007.07.018 - Pubmed citation
2017.3.15
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.