

Clinical diagnosis
Case 47
They were given antibiotics for a few days and non-steroid anti-inflammatory drug until abating pain.
【Discussion】
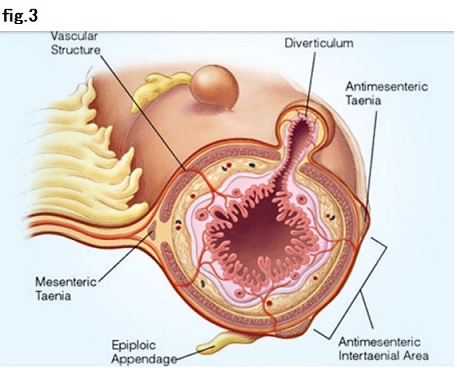
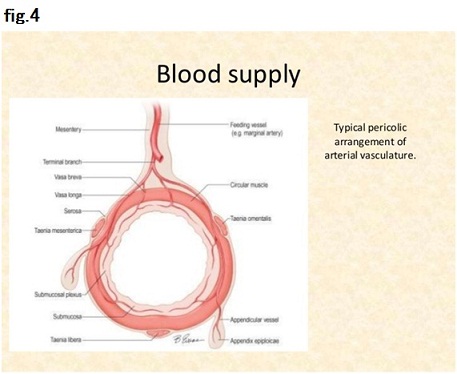
Epiploic appendages are small fatty pouches connected with subserous tissue of the colon (Figs 3, 4). They are appended to the entire colon except rectum. Their function is not known. They are usually arranged in two rows along with colon tania. Their average size was 3.0 cm (0.5 – 5) (1-11). It is hard for normal epiploic appendages to be detected in routine abdominal CT but occasionally detected in case of massive ascitis and/or mesentery inflammation.
Obesity is the predisposing factor to epiploic appendagitis which is categorized according to its cause. The main cause is blood flow disorder (approximately 80%), indicating ischemic infarction due to torsion which is probably caused by the fat-deposit weighty epiploic appendages (1-5). Actually, the neck of the weighty epiploic appendage is narrow and susceptible to torsion. Each epiploic appendage has paired arteries and single vein (Fig. 4). Then, venous occlusion is first, affected. Other causes are hernia incarceration, intestinal obstruction, and intraperitoneal loose body.
Histological findings revealed that congestion of fat tissue accompanied with hemorrhagic infarction at the initial stage followed by inflammatory response, inducing finally to fibrotic calcified organization (5). CT findings reflect the pathological findings that ring rim (hyperattenuating ring sign) outlining the oval fat tissue indicates the inflamed thickening of peritoneum surrounding an epiploic appendage, spotty high attenuation inside the oval fat indicates venous thrombosis and/or hemorrhagic infarction and trabecular pattern such as dirty fat sign indicates the inflammatory edema. The wall of the adjacent colon is most often normal in thickness (6-11).
Clinical symptoms of epiploic appendagitis are localized peritonitis which occur at any location of the whole abdomen, but abdominal pain largely occur at the right or left lower abdomen because cecum/ascending colon and sigmoid colon is predisposing. Pain occurs sometimes during/after defecation. Of the reported surgically resected cases, ascending colon (38%) and sigmoid colon (36%) are the most, followed by transverse colon (13%), cecum (9%) and descending colon (2%) (8).
Acute epiploic appendagitis is most managed conservatively using non-steroid anti-inflammatory druds and antibiotics are not always necessary, depending on the results of laboratory test (4, 5). The symptoms are self-limited and the pain relief is obtained in less than 10 days.
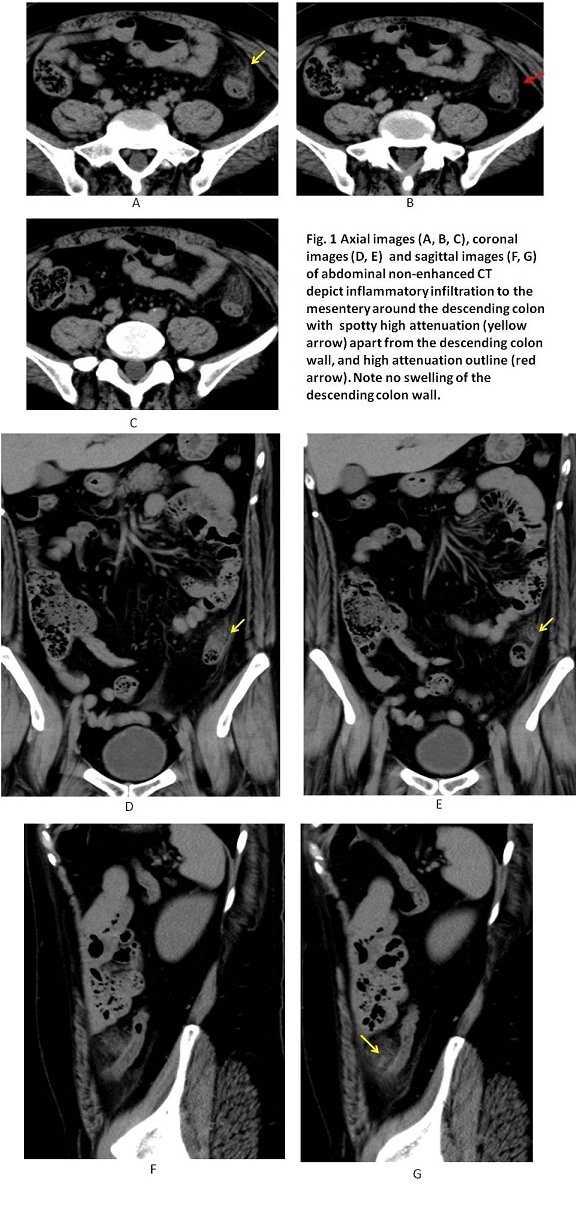
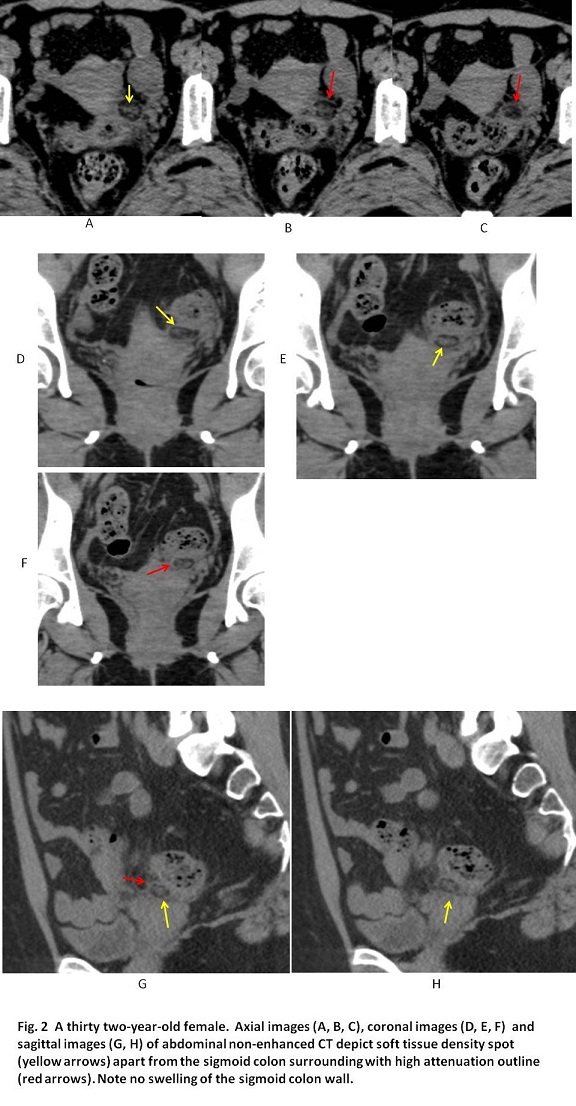
Our two cases owned thick subcutaneous fat, suffering from lower abdominal pain, left lower abdominal pain in each, and their non-enhanced CT showed oval fat density with high attenuation ring sign and spotty high attenuation inside the oval fat density in the descending colon and sigmoid colon, corresponding to the typical images of epiploic appendagitis.
【Summary】
We present two cases with epiploic appendagitis that CT showed oval fat density with high attenuation margin and spotty high attenuation inside, indicating the inflamed thickening of peritoneum surrounding an epiploic appendage and venous thrombosis and/or hemorrhagic infarction, respectively. Although their symptoms are self-limited, antibiotics and non-steroid anti-inflammatory drug were given. We should keep in mind the typical images of epiploic appndagitis; oval fat density with high attenuation margin and spotty high attenuation inside as one of the major three diseases causing abdominal pain (other two diseases: appendicitis, diverticulitis).
【References】
1.Sand, M., et al. Epiploic appendagitis – clinical characteristics of an uncommon surgical diagnosis. BMC Surgery. 2007 7:11
2.van Breda Vriesman AC:The hyperattenuating ring sign. Radiology 2003; 226: 556–557.
3.RosenMP, et al. Value of abdominal CT in the emergency department for patients with abdominal pain. Eur Radiol2003; 13(2): 418–424. Medline
4.CarmichaelDH, et al. Epiploic disorders: conditions of the epiploic appendages. Arch Surg1985; 120: 1167–1172. CrossRef, Medline
5.LynnTE, et al. A clinico-pathologic study of the epiploic appendages. Surg Gynecol Obstet1956; 103: 423–424. Medline
6.DanielsonK, et al. Epiploic appendagitis: CT characteristics. J Comput Assist Tomogr1986; 10: 142–143. CrossRef, Medline
7.SinghAK, et al. CT of acute appendagitis. AJR Am J Roentgenol2004; 183: 1303–1307. CrossRef, Medline
8.ZissinR, et al. Acute epiploic appendagitis: CT findings in 33 cases. Emerg Radiol2002; 9(5): 262–265. Medline
9.SonHJ, et al. Clinical diagnosis of primary epiploic appendagitis: differentiation from acute diverticulitis. J Clin Gastroenterol 2002; 34(4): 435–438. CrossRef, Medline
10.SandrasegaranK, et al. Primary epiploic appendagitis: CT diagnosis. Emerg Radiol 2004; 11: 9–14. Medline
11.RaoPM, et al. Primary epiploic appendagitis: evolutionary changes in CT appearance. Radiology1997; 204(3): 713–717. Link
2017.3.22
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.