

The appropriate choice
Case 56
【Angiography and embolization】
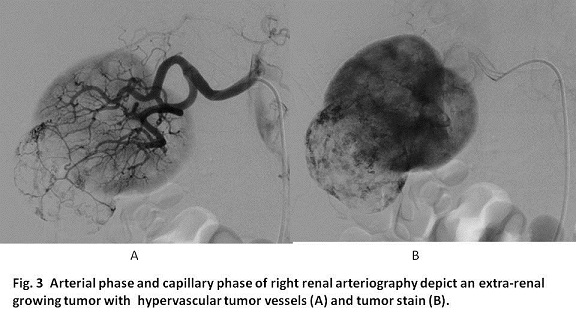
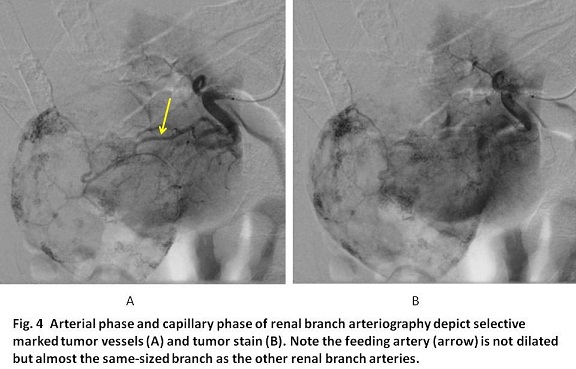
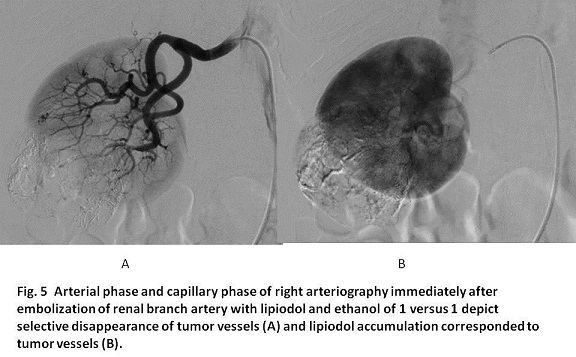
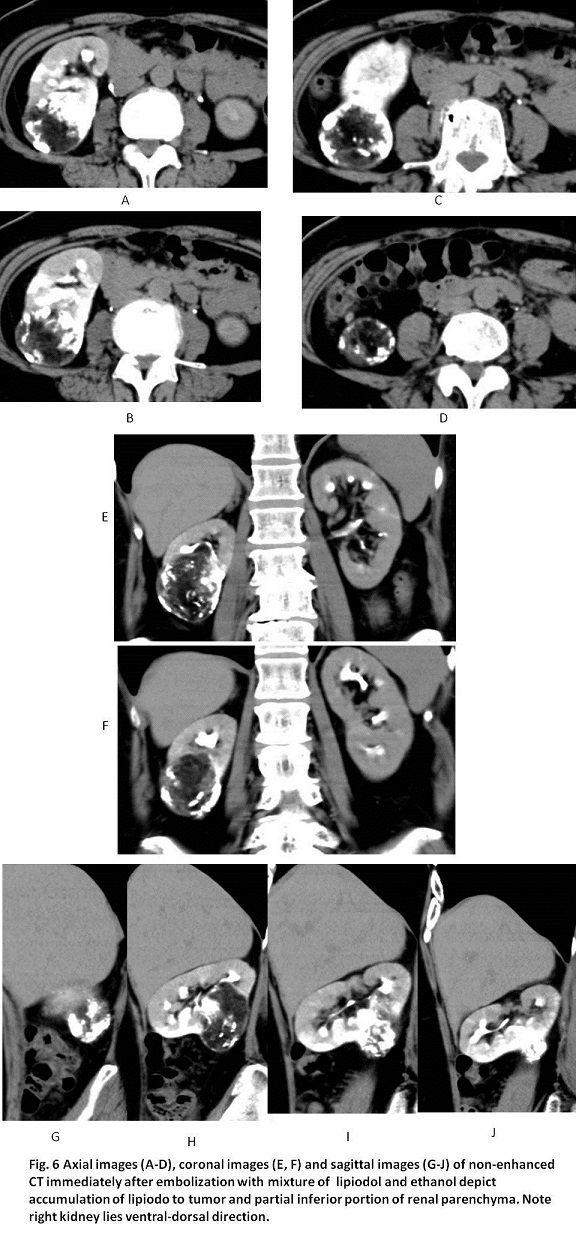
Right renal arteriography using a 3F catheter system showed a hypervascular tumor growing extra-renally which probably made a right kidney rotated from cranial-caudal position to ventral-dorsal position (Fig. 3). A 2F microcatheter was inserted to the right renal branch artery whose arteriography showed marked tumor stain and the feeding artery (Fig. 4). The microcatheter was advanced using a 0.014 micro-guidewire to the feeding artery. The mixture of ethanol and lipiodol (1 versus 1) was created. Before embolization, analgetics was intravenously infused and 10 ml of xylocaine was infused via the microcatheter. Under fluoroscopic guidance, embolization with lipiodol and ethanol was conducted. Immediately after embolization, right renal arteriography showed selective disappearance of tumor stain (Fig. 5). Non-enhanced CT after embolization showed lipiodol accumulation to the tumor and surrounding renal parenchyma (Fig. 6).
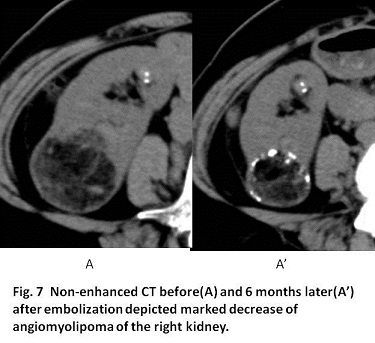
Immediately after embolization, she felt slight backache for several hours. She experienced slight fever for a few days. Five days later, she discharged without complication and returned home in a healthy condition. Six months later, non-enhanced CT showed marked decrease of angiomyolipoma of the right kidney (Fig. 7).
Angiomyolipoma (AML) of the kidney is a benign neoplasma histologically composed of smooth muscle, lipid and vascular tissue. The vascular tissue is prone to form aneurysms, inducing rupture. In the literature, Renal AVM occurs with the incidence of 0.3 to 3 % of the population (1), 90 % of AML which occur spontaneously are unilateral and solitary, while 10 % which are associated with tuberous sclerosis or pulmonary lymphanioleiomyomatosis are bilateral and/or multiple (1, 2). Factors with risk of hemorrhage are listed; greater than 4 cm in diameter with 100 % sensitivity and 40 % specificity to predict rupture (3, 4); aneurysm size greater than 5 mm; AVM with tuberous sclerosis than spontaneous AVM (3 – 7). In our case, she had solitary AML sized 4.5 cm with no association with tuberous sclerosis and pulmonary lymphangioleiomyomatosis. Her AML was increasing the size of 0.2 cm in a year with extra-renal growth.
As treatments for AML, surgical partial nephrectomy, radiofrequency ablation, microwave coagulation, cryoablation and renal artery embolization are listed. Of these, renal artery embolization (RAE) is most supplied because of the less invasive and timely hemostasis for acute hemorrhage from AML. Further, as prophylactic treatment, RAE is reasonable to selectively occlude the vascular component responsible for hemorrhage. However, up to 5 % of initial embolization requires a repeat embolization (8 -10). In Japan, gelatin sponge particles have been used for embolization for AML. Gelatin sponge is known to be absorbed as the organization process for foreign body in the vessel. As a result, the narrowing reopening of the occluded artery can occur. In the USA, polyvinyl alcohol particles or tri-acryl microspheres which are inert (not absorbed), are being used (11). The ideal embolic material is absolute ethanol, inducing eradication of all AML components (12). Actually ethanol was once used for preoperative management for renal cell cancer. However, ethanol is not visible under fluoroscopic guidance with higher risk of renal parenchyma damage due to reflux of ethanol. Then, an occlusion balloon catheter was considered to be essential for ethanol embolization (12). It is not problematic for total occlusion of renal artery for renal cell carcinoma since the balloon catheterization to the renal artery was not difficult and the kidney with renal cell carcinoma was finally removed. However, in case of AML for prophylactic treatment, kidney damage should be as least as possible. For that, an occlusion balloon catheter has to advance as close to the feeding artery as possible.
In our case, the kidney was rotated from cranial-caudal axis to ventral-dorsal axis, causing the difficulty to identify the feeding artery. The diameter of the feeding artery for AML was the same diameter or rather thin compared to that of normal renal branch arteries. This situation was different from the situation of ethanol embolization for renal cell cancer because renal branch artery feeding renal cell carcinoma is dilated compared to the intact renal branch arteries. The thin diameter of the feeding artery indicated a bit difficulty in the selective insertion of the occlusion balloon catheter to the feeding artery. Then, in order to overcome these problems, we used the mixture of ethanol and lipiodol as the embolic material via the microcatheter advanced as close as possible to the feeding artery. The dynamics of the mixture can be seen in radio-fluoroscopic guidance and the infusion of the mixture is reported to be potent enough to eradicate arteriovenous malformation (13). As a result, non-enhanced CT after embolization depict almost selective accumulation of lipiodol to the entire AML and the surrounding renal parenchyma.
【Summary】
We present a sixty five-year-old female with angiomyolipoma sized 4.5 cm with the annually growing which was successfully treated by prophylactic renal branch artery embolization with the mixture of ethanol and lipiodol with the ratio of 1 : 1. The selective catheterization to the feeding artery, one of the renal branch arteries was a bit difficult because the right kidney was rotated from cranial-caudal axis to ventral-dorsal axis and the feeding artery is thinner rather than the normal renal branch arteries. Following embolization, non-enhanced CT showed selective accumulation of lipiodol to the AML and the surrounding renal parenchyma. Six months later, non-enhanced CT showed marked decrease of angiomyolipoma of the right kidney. Embolization with the mixture of ethanol and lipiodol for AML was safe and effective, although it is yet to be reported.
【References】
1.Fittschen A, et al. Prevalence of sporadic renal angiomyolipoma: a retrospective analysis of 61,389 in- and out-patients. Abdom Imaging. 2014; 39:1009-13. | Article | PubMed
2.Bissler JJ, et al. Reduction of postembolization syndrome after ablation of renal angiomyolipoma. Am J Kidney Dis. 2002; 39:966-71. | Article | PubMed
3.Lai HY, et al. Multicentric aggressive angiomyolipomas: a rare form of PEComas. AJR Am J Roentgenol. 2006; 186:837-40. | Article | PubMed
4.Cui L, et al. CT imaging and histopathological features of renal epithelioid angiomyolipomas. Clin Radiol. 2012; 67:e77-82. | Article | PubMed
5.Rimon U, et al. Large renal angiomyolipomas: digital subtraction angiographic grading and presentation with bleeding. Clin Radiol. 2006; 61:520-6. | Article | PubMed
6.Krueger DA et al. Tuberous sclerosis complex surveillance and management: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013; 49:255-65. | Article | PubMed Abstract | PubMed FullText
7.Rouviere O, et al. Kidney damage due to tuberous sclerosis complex: management recommendations. Diagn Interv Imaging. 2013; 94:225-37. | Article | PubMed
8.Yamakado K, et al. Renal angiomyolipoma: relationships between tumor size, aneurysm formation, and rupture. Radiology. 2002; 225:78-82. | Article | PubMed
9.Johnson SR, et al. European Respiratory Society guidelines for the diagnosis and management of lymphangioleiomyomatosis. Eur Respir J. 2010; 35:14-26. | Article | PubMed
10.Hamlin JA, et al. Renal angiomyolipomas: long-term follow-up of embolization for acute hemorrhage. Can Assoc Radiol J. 1997; 48:191-8.
11.Hocquelet A, Cornelis F, Le Bras Y, Meyer M, Tricaud E, Lasserre AS, Ferriere JM, Robert G and Grenier N. Long-term results of preventive embolization of renal angiomyolipomas: evaluation of predictive factors of volume decrease. Eur Radiol. 2014; 24:1785-93. | Article | PubMed
12.Takebayashi S, Horikawa A, Arai M, Iso S and Noguchi K. Transarterial ethanol ablation for sporadic and non-hemorrhaging angiomyolipoma in the kidney. Eur J Radiol. 2009; 72:139-45.
13.Kawai N, et al. Prostate-supplying arteriogram created by multidetector-row CT during pelvic arteriography: contribution to the treatment strategy of prostatic artery embolization for prostatic hyperplasia. Jpn J Radiol 32(8): 491-495, 2014
2017.5.31