

Clinical diagnosis
Case 57
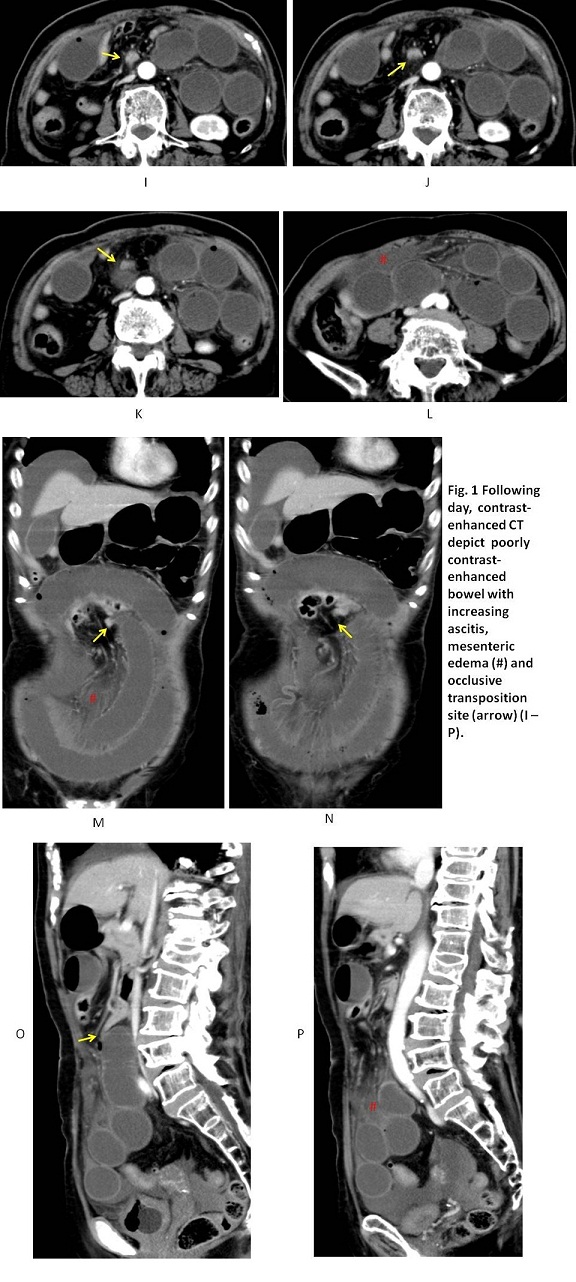
【Following day】
The patient of Case 1 experienced increasing abdominal pain and hypotension, and contrast-enhanced CT showed increasing ascitis, mesenteric edema and poorly contrast-enhanced small bowel, fearing bowel ischemic damages (Fig.1 I – P). She received laparatomy which revealed strangulation ileus with necrotic small bowels. The patient of Case 5 was transported to the other hospital where laparotomy and resection of small bowel were conduced.
【Discussion】
When small bowel obstruction is encountered, it is imperative to diagnose whether there exists strangulation ileus or not. In general, as a clinical treatment strategy for symptomatic ileus, gastric or intestinal tube insertion is first conducted to decrease internal pressure and then, the careful clinical observation including laboratory test is crucial. When symptoms worsen such as occurrence of peritonitis and sudden hypotention, surgical management is often determined. For strangulation ileus, the sooner exact diagnosis brings the better outcome. In Case 1, the following day after non-enhanced CT (Fig. 1 A – H), she fell into a sub-shock state and contrast-enhanced CT showed poorly enhanced small bowels, implying bowel necrosis. In Case 5, because ascitis increased the following day (Fig. 5 D, E, F) and abdominal pain continued, surgical management was determined, revealing necrosis of small bowels.
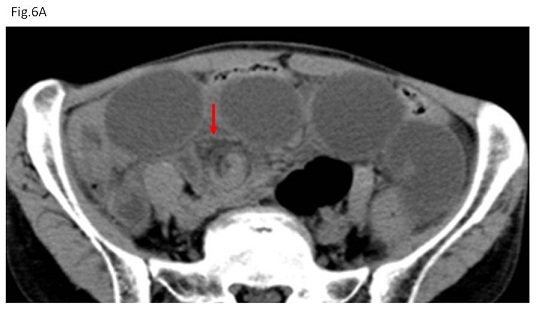
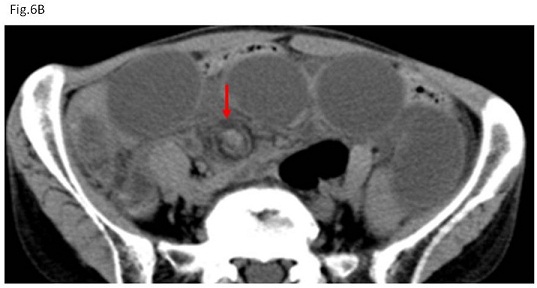
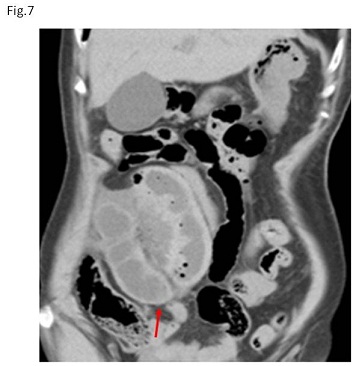
Abdominal CT is known to contribute to early diagnosis of strangulation ileus. The typical findings of strangulation ileus on CT are known to be whirl sign, beak sign (Fig. 6) and closed loop sign (Fig. 7) (1 – 4). Whirl sign indicates the small bowel turns around the mesenteric vessels (Fig 6), beak sign indicates the small bowel occludes at the edge of the beak configuration (Fig. 6) and loop sign indicates round loop in the closed space (Fig. 7) (4) which is usually visualized on coronal images because the coronal space of the abdomen is wider than axial or sagittal space.
Non-enhanced CT of Case 2 showed small bowel rotated around mesenteric vessels that edge of the beak configuration was not occluded but slightly opening (Fig. 2 B-E), implying the loose occlusive transposition site. Non-enhanced CTs of Cases 3 to 5 (Figs 3 – 5) showed no existence of whirl sign, beak sign and closed loop sign and they showed that the contracted bowel and dilated small bowel nestled together. Meanwhile, non-enhanced CT of Case 1 showed highly tightening of contracted small bowel edge, mesenteric edema and ascitis, although whirl sign was unclear and the edge of the contracted small bowel was not closed. Ascitis itself is an unfavorable situation and not a determinant finding for laparotomy. However, in Case 1 and 5 (Fig. 5), symptoms of abdominal pain worsened with increasing ascitis. Laparomy revealed necrosis of small bowel due to strangulation ileus. Ileus associated with mesenteric edema indicates the compression of the mesentery, namely portal vein occlusion but not always artery occlusion. Mesenteric edema implies more occlusive strength of mesentery than ileus without mesenteric edema. In fact, non-enhanced CT of Case 3 indicated ileus with mimicking mesenteric edema but no evidence of ascitis inducing no surgical management. Meanwhile, non-enhanced CT of Case 1 showed mesenteric edema plus ascitis that imply the more tightening situation than the situation with mesenteric edema alone or the situation with ascitis alone.
The most crucial point is whether small bowel necrosis was caused by ileus or not. Contrast-enhanced CT is preferable to conduct whether the dilated small bowel gets enough blood supply or not. However, contrast-enhanced CT is sometimes limited to use because of renal dysfunction and/or iodine allergy (5). Of our five cases, two patients of Case 1 and Case 5 (enhanced CT of Case 5 is not listed) received contrast-enhanced CT which showed poorly enhancement. Contrast-enhanced CT should be conducted in cases of ileus with ascitis.

【Summary】
We present five cases with ileus whose non-enhanced CT showed no evidence of whirl sign, beak sign and closed loop sign except case2. Of the five patients, two patients of Case 1 and 5 received laparotomy on the following day that revealed strangulation ileus with necrotic small bowel. Three radiological findings of highly tightening of contracted small bowel, metenteric edema and increasing asitis might be crucial for determinant factors for small bowel ischemic change. We should keep in mind if two or three of these findings are found on non-enhanced CT, the strangulation ileus possibly occurs even if there were no typical findings of whirl sign, beak sign or closed loop sign.
【References】
1.Duda JB, Bhatt S, Dogra VS. Utility of CT whirl sign in guiding management of small-bowel obstruction. AJR Am J Roentgenol 2008;191:743-747.
2.Khurana B. The whirl sign. Radiology 2003:226:69-70.
3.De Korte N, Grutters CT, Snellen JP. Small bowel volvulus diagnosed by the CT ‘whirl sign’. J Gastrointest Surg 2008:12(8):1469-1470. Epub 2007 Oct 20.
4.Owuagwu O, et al. Small bowel volvulus: a review. J R Coll Surg Edinb 1999;44:150-155.
5.5. Guidelines for Intravenous Iodinated Contrast Administration in Outpatients Computed Tomography Examinations. https://radiology.ucsf.edu/patient-care/.../contrast/.../elevated-creatin.
2017.6.7