

The appropriate choice
Case 58
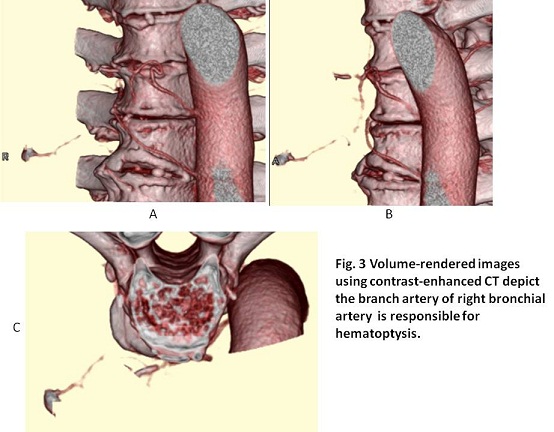
Before angiography, volume-rendered (VR) images were created using contrast-enhanced CT aquisition data to investigate the relation of hemorrhage with responsible artery. It showed the responsible artery is a branch artery of the right bronchial artery (Fig. 3). The branching site of the right bronchial artery from thoracic aorta was confirmed in VR images.
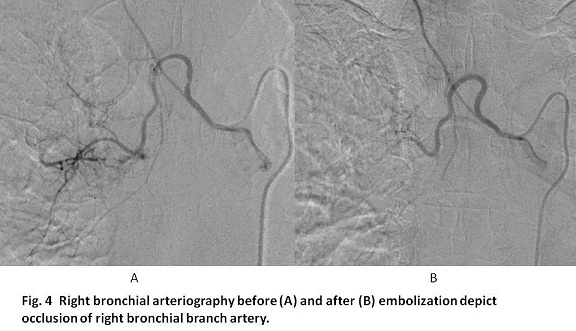
Right bronchial arteriography using a 3F Mikaellson catheter was first conducted (Fig. 4A). Then, a microcatheter via the 3F catheter was advanced to the branch artery responsible for hemosputum. Beonchial artery embolization (BAE) was conducted with gelatin sponge particles that were made of sliced Spongel into 1 to 2 mm in pieces with a small scissor and soaked with contrast medium. After BAE, bronchial arteriography showed selective occlusion of bronchial branch artery (Fig. 4B).
【Progress】
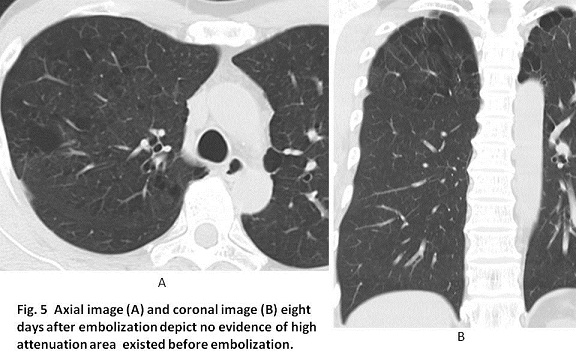
He was discharged two days later because hemosputum did not come out. Non-enhanced CT eight days after BAE showed no high attenuation in the right upper lobe (Fig. 5). He has not experienced hemosputum for 10 months since he underwent BAE.
【Discussion】
When gelatin sponge particles (GSPs) sliced into 1 mm in size are infused in a bronchial artery, GSPs can reach to the small branch arteries sized 100 μm or greater because they are so flexible and contractile that they can pass through to the smaller arteries than their own sizes (1). Microscopically, GSPs are net-like configuration and own open spaces that are occupied with red thrombus in the embolized vessels, completing the occlusion of the vessel lumen. GSPs stayed in the vessel are organized and absorbed with infiltration of histiocytes coming from smooth muscle layer of the vessel (1). It induces occlusion, stenosis or recanalization of the vessel. When recanalization of the vessel occurs, hemosputum might reoccur after BAE with GSPs (2 -4). However, at the same time, BAE with GSPs prevents the growth of collateral development from the systemic arteries except bronchial artery, implying repeated BAE is not difficult.
The configuration of polyvinyl alcohol is similar as GSPs but polyvinyl alcohol is inflexible and least contractile, indicating BAE with polyvinyl alcohol induces the more proximal occlusion. Further, polyvinyl alcohol is not absorbed but permanent in the vessel, inducing collateral development from systemic arteries such as thoracic artery, intercostals and intra-thoracic arteries. Hemosputum reoccurs from the development of collaterals implies the difficult catheter management on catheter insertion. BAE with microcoils induces the same situation as BAE with polyvinyl alcohol. Namely, microcoils are permanent, proximal and cost-expensive embolic materials.
When mixture of n-butyl cyanoacrylate (NBCA) and lipiodol with the ratio of 1 : 7 is infused in the bronchial artery, NBCA can reach to the vessel of 100 μm or greater in size which indicates relatively peripheral embolization such as GSPs (1). BAE with NBCA owns more occlusive potency than that with GSPs (5, 6). However, skill-master curve is required to handle NBCA for embolization. The excessive volume of NBCA regurgitate to aorta, causing unexpected complication. Infusion of mixture of ethanol with lipiodol is contra-indicative because ethanol itself possibly causes the bronchial wall damage. In our case, the bronchial branch artery responsible for hemosputum is not dilated. We considered that BAE with gelatin sponge particles is safe because a small volume of embolic material seems to be sufficient. As a result, of these embolic materials, BAE with GSPs are the most preferable.
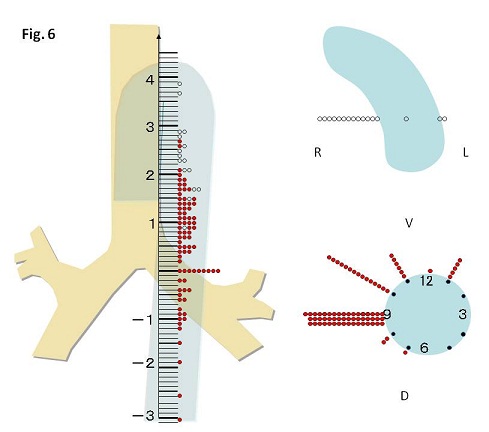
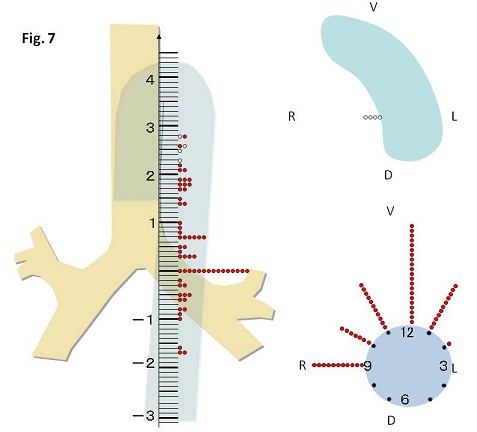
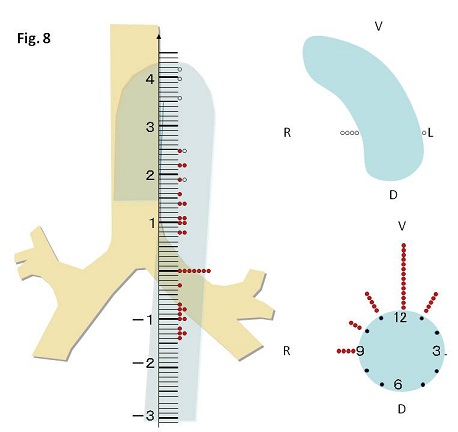
As background knowledge for BAE, anterior spinal artery possibly communicates with bronchial artery. The anterior spinal artery branched from vertebral artery connect with Adamkiewicz artery which branches from radicular branch of lower intercostals artery. Right bronchial artery is known to often branch from the common tract of right intercostals artery mostly at the level of bronchial bifurcation (Figs.6-8) (7). Therefore, there is possible communication between right bronchial artery and anterior spinal artery, indicating embolization from the proximal site of bronchial artery possibly causes paraplegia. When BAE is attempted via a microcatheter, the microcatheter should be advanced beyond the inlet of radicular branch artery, namely beyond the margin of thoracic vertebra, even if bronchial artery does not communicate with intercostals artery.
【Summary】
We present a fifty two-year-old male with persistent hemoptysis for several days despite coagulants medicine intake which was successfully managed by bronchial arterial embolization (BAE) with gelatin sponge particles (GSPs). We should keep in mind that when bronchial artery is catheterized to the right bronchial artery, a microcatheter has to be advanced over right margin of thoracic vertebra body under radiologic fluoroscopic guidance to avoid the possible branch of anterior spinal artery. Further, GSPs of 1 mm in size can reach to the small branch arteries sized 100 μm or greater, and occluded arteries after BAE with GSPs can be re-opened, but remaining narrowing lumen and the less development of collaterals.
【References】
1.anaka T, et al. Safety of bronchial arterial embolization with n-butyl cyanoacrylate in a swine model. World J Radiol 4(12): 455-461, 2012
2.Remy J, et al. Treatment of hemoptysis by embolization of the systemic circulation . Ann Radiol (Paris) 1974; 17: 5-16
3.Uflacker R, et al. Bronchial artery embolization in the management of hemoptysis: technical aspects and long-term results. Radiology 1985; 157:637-644.
4.Hayakawa K, et al. Bronchial artery embolization for hemoptysis: immediate and long-term results. Cardiovasc Intervent Radiol 1992; 15: 154-158.
5.Kawai N, et al.: Bronchial artery aneurysm and pulmonary arteriovenous malformation. J Vasc Interv Radiol 24(1): 47, 2013
6.Ikoma A, et al. Pathologic evaluation of damage to bronchial artery, bronchial wall, and pulmonary parenchyma after bronchial artery embolization with N-butyl cyanoacrylate for massive hemoptysis. J Vasc Interv Radiol 22(8): 1212-1215, 2011
7.Ziyawudong J,et al. Aortic ostia of the bronchial arteries and tracheal bifurcation: MDCT analysis. World J Radiol 4(1): 29-35, 2012
2017.6.14
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.