

Clinical diagnosis
Case 59
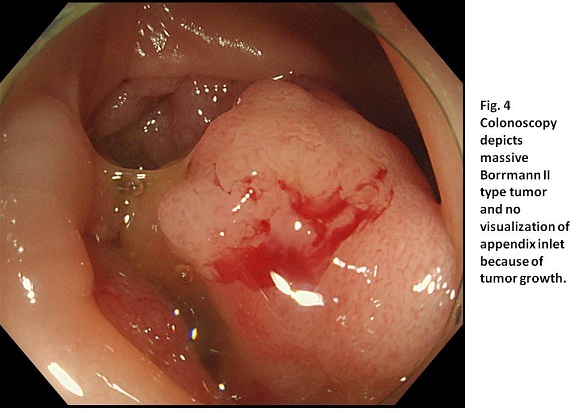
Colon endoscopy revealed advanced cancer at the cecum (Fig. 4). The orifice of the appendix could not be found because it was hidden by the existence of the tumor.
【Progress】
After colonoscopy, she underwent laparotomy to remove cecum cancer whose macroscopic specimen showed Borrmann II type advanced carcinoma. She was scheduled to be given chemotherapy. One month later, the first-line chemotherapy was initiated.
【Discussion】
Of the entire colorectal cancers, cecum is one of the common sites for cancer to arise: 25% on the right-side colon (cecum, ascending colon, and transverse colon), 4% in the splenic flexure, 25% on the left-side colon, and 45% in the sigmoid colon and rectum (1. 2). As well as other colorectal cancers, cecum cancer causes anemia and constipation because it often ulcerates, bleeds and massively grows. Cecum cancer can cause appendicitis more often rather than the other colorectal cancers. Obstruction of appendix orifice is known to occur in one of the three ways; tumor adjacent to appendix; inflammation by the cecum carcinoma; tumor of the colon causing back pressure and consequent obstruction of the appendix (3). In our case, the growth of cecum cancer blocks the orifice of appendix, inducing inflammation to the appendix, ascending colon and ileum. In general, acute appendicitis in children and young adults results from luminal obstruction by fecalith and/or lymphoid hypertrophy (4). Meanwhile, acute appendicitis in elderly adults is known to result from cecum cancer with the incidence of 10 to 25 % (5, 6) [from ascending colon cancer + cecum cancer, 4 to 15 % (2), from entire colon cancer, 1.8 to 8 % (7-9)]. We should keep in mind that the coexistence of cecal cancer and acute appendicitis is not so rare in elderly patients.
Back to our case for verification, non-enhanced CT on Day 1 showed colitis, enteritis and appendicitis with cecum thick density mimicking swollen Baufin valve which was interpreted as cecum inflammation. Then, it was considered that surgical management for appendicitis should be avoided because of the possible difficulty of anastomosis due to the cecum inflammation. The patient started to be given intravenous antibiotics. Contrast-enhanced CT on Day 3 showed more severe degree of colitis, enteritis and appendicitis with much water-like content and swollen walls of the ascending colon, intestine and appendix. It was still considered the surgical management should be avoided because of existence of the severe inflammation. The patient was continued to be given intravenous medicine adding new antibiotics. However, on Day 5, the patient’s symptoms were becoming worse than ever. Non-enhanced CT showed the more dilated appendix, misgiving the rupture. Colonoscopy showed cecum cancer obstructing the orifice of the appendix. From a point of retrospect view, the earlier conduct of colonoscopy such as Day 2 or Day 3 might have been the favorable choice. Although enhanced CT showed all aspects of the lesions of ascending colon, cecum, appendix and ileum, the image interpretation was not easy to differentiate cecum cancer from swollem cecum inflammation.
【Summary】
We present a fifty two-year-old female with coexistence of colitis, ileitis and appendicitis caused by cecum cancer. From retrospective, CT showed cecum cancer blocked the orifice of the appendix which was confirmed by colonoscopy. We should keep in mind that appendicitis in elderly patients is caused by cecum cancer with the relatively high incidence of 10 to 20 %.
【References】
1.Winawer S, et al. Colorectal cancer screening and surveillance: clinical guidelines and rationale-update based on new evidence. Gastroenterology 2003; 124:544-560.
2.Lai HW, et al. Incidence and odds ratio of appendicitis as first manifestation of colon cancer: a retrospective analysis of 1873 patients. J Gastroenterol Hepatol. 2006 Nov;21(11):1693-6.
3.Michowitz M, et al. Perforation complicating carcinoma of colon. J Surg Oncol. 1982 Jan;19(1):18-21.
4.Collins DC : Etiologic factors in acute appendicitis based upon study of 3,400 cases. Surgery 1939; 5 : 267-270.
5.Patterson JF Jr et al. Carcinoma of the cecum. Am J Surg. 1951; 81 : 618-621.
6.Hellsten H et al. Coexistent cecal cancer and appendicular abscess. Arch Surg 1951; 62 : 112-117
7.Bizer LS. Acute appendicitis is rarely the initial presentation of cecal cancer in the elderly patient. J Surg Oncol. 1993;54:45–46. [PubMed]
8.Bleker RJ, Wereldsma JC. Colonic malignancy mimicking an appendiceal mass. Neth J Surg. 1989;41:42–46. [PubMed]
9.Poon RT, Chu KW. Inflammatory cecal masses in patients presenting with appendicitis. World J Surg. 1999;23:713–716. doi: 10.1007/PL00012374. [PubMed] [Cross Ref]
2017.6.21
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.