

Probable diagnosis
Case 92
【Progress】
He was admitted to our hospital for observation and rehabilitation. His Barre’s arm sign was positive of left upper extremity. Electroencephalogram (EEG) revealed small spikes at right front-parietal area of his brain. Because his symptoms were not advanced, he was discharged seven days later.
【Discussion】
β amyloid protein is one of waste products from neuron, and largely divided into β amyloid (βA) 40 and βA 42. βA 42 aggregates and deposits in the brain parenchyma, causing Alzheimer disease (1, 2). βA 40 does not easily aggregates and is transported through periarterial interstitial fluid drainage called glymphatic system, to blood vessels for clearance. As a result, βA 40 accumulates in the vessel wall itself, first on vascular outer basement and deposits in the outer regions of the media and adventitia but not in intima. The accumulation of βA 40 in the smooth muscle of the media induces fragility, weakness and fibrinoid necrosis of vascular wall, leading to microbleeds. Further, amyloid β infiltrates the surrounding parenchyma and damages neuron, inducing dystrophic neurites (1, 2).
Cerebral amyloid angiopathy is observed in leptomeningeal and cortical vessels of cerebral lobes (occipital lobe, the most) and cerebellum but not in basal ganglion, thalamus, brain stem and white matter. This is one of the major differences between cerebral amyloid angiopathy and hypertensive angiopathy. Cerebral amyloid angiopathy causes various hemorrhagic lesions: lobar intracerebral macro-hemorrhage, microbleeds, and subarachnoid hemorrhage/cortical superficial (hemo)siderosis. Of the intracerebral hemorrhages, cerebral amyloid angiopathy is the second most following hypertensive intracerebral hemorrhage. Further, it causes ischemic lesions: cortical infarction and ischemic changes of white matter. Furthermore, it causes angitis by antibody to amyloid protein: subacute leukoencephalopathy which is predominantly found in the occipital lobe. Microbleeds are noted in 17-32 % of Alzheimer patients and 5-6 % of normal population (3-6). Namely, cerebral amyloid angiopathy induces cerebral hemorrhage, infarction, leukoencephalopathy and dementia.
In our case, brain MRI showed microbleeds, cortical hemorrhagic infarction and cortical superficial siderosis. It is known that cortical superficial siderosis present with transient focal neurological episodes, being a clinical marker of this disease (7-11). Our patient suffered from repeated transient paresis of left upper arm which matched with cortical superficial siderosis spreading, irritating and depressing.
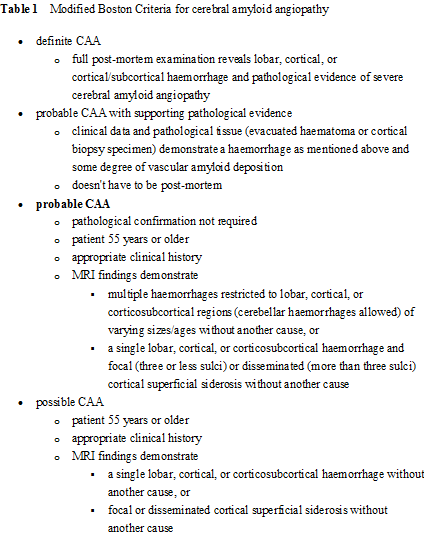
As risk factors of cerebral amyloid angiopathy, aging and Alzheimer disease are listed. According to modified Boston criteria for cerebral amyloid angiopathy (Table 1), our case matched with probable CAA without requiring pathological confirmation; 74 years old > 55 years or older; recurrent transient hemiparesis, appropriate clinical history; multiple microbleeds, cortical superficial siderosis, hemorrhage restricted to right parietal lobe on MRI findings.
【Summary】
We present a seventy four-year-old male suffering from recurrent left arm palsy. Brain MRI showed multiple microbleeds, local cortex bleeding at right parietal lobe and multiple cortical superficial siderosis. His clinical data, symptom and MRI findings matched with probable cerebral amyloid angiopathy of modified Boston criteria. We should keep in mind that cerebral amyloid angiopathy (cortical superficial hemosiderosis) present with transient neurological episodes, and causes various hemorrhage: intracranial hemorrhage, local microhemorrhage, microbleeds and cortical superficial hemosiderosis, and infarctions. Further, β amyloid (βA) 40 and βA 42 are related to the onset of amyloid angiopathy and Alzheimer disease, respectively. βA 42 accumulate in brain parenchyma , inducing Alzheimer disease and βA 40 is transported to the vessel walls, inducing amyloid angiopathy.
【References】
1.Yamada M, et al. Cerebral Amyloid Angiopathy: Emerging Concepts. J Stroke. 2015 Jan; 17(1): 17–30. Published online 2015 Jan 30. doi: 10.5853/jos.2015.17.1.17 PMCID: PMC4325636
2.Anand Viswanathan, et al. Cerebral Amyloid Angiopathy in the Elderly. Ann Neurol. 2011 Dec; 70(6): 871–880. doi: 10.1002/ana.22516 PMCID: PMC4004372 NIHMSID: NIHMS573907
3.Hanyu H, Tanaka Y, Shimizu S, Takasaki M, Abe K. Cerebral microbleeds in Alzheimer's disease. J Neurol. 2003;250:1496–1497. [PubMed]
4.Nakata-Kudo Y, Mizuno T, Yamada K, Shiga K, Yoshikawa K, Mori S, et al. Microbleeds in Alzheimer disease are more related to cerebral amyloid angiopathy than cerebrovascular disease. Dement Geriatr Cogn Disord. 2006;22:8–14. [PubMed]
5.Cordonnier C, van der Flier WM, Sluimer JD, Leys D, Bark hof F, Scheltens P. Prevalence and severity of microbleeds in a memory clinic setting. Neurology. 2006;66:1356–1360. [PubMed]
6.Cordonnier C, Al-Shahi Salman R, Wardlaw J. Spontaneous brain microbleeds: systematic review, subgroup analyses and standards for study design and reporting. Brain. 2007;130:1988–2003. [PubMed]
7.Izenberg A, Aviv RI, Demaerschalk BM, Dodick DW, Hopyan J, Black SE, et al. Crescendo transient aura attacks: a transient ischemic attack mimic caused by focal subarachnoid hemorrhage. Stroke. 2009;40:3725–3729. [PubMed]
8.Beitzke M, Gattringer T, Enzinger C, Wagner G, Niederkorn K, Fazekas F. Clinical presentation, etiology, and long-term prognosis in patients with nontraumatic convexal subarachnoid hemorrhage. Stroke. 2011;42:3055–3060. [PubMed]
9.Charidimou A, Peeters A, Fox Z, Gregoire SM, Vandermeeren Y, Laloux P, et al. Spectrum of transient focal neurological episodes in cerebral amyloid angiopathy: multicentre magnetic resonance imaging cohort study and meta-analysis. Stroke. 2012;43:2324–2330. [PubMed]
10.Apoil M, Cogez J, Dubuc L, Bataille M, de la Sayette V, Touzé E, et al. Focal cortical subarachnoid hemorrhage revealed by recurrent paresthesias: a clinico-radiological syndrome strongly associated with cerebral amyloid angiopathy. Cerebrovasc Dis. 2013;36:139–144. [PubMed]
11.Charidimou A, Baron JC, Werring DJ. Transient focal neurological episodes, cerebral amyloid angiopathy, and intracerebral hemorrhage risk: looking beyond TIAs. Int J Stroke. 2013;8:105–108. [PubMed]
2018.2.14
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.