

Clinical diagnosis
Case 10
【Clinical progress】
Blood culture test revealed infection of Fusobacterium nucleatum. He was given metronidazole (Furazyl) changing from penicillin, dramatically improving the shrinkage of the abscess and the empyema. Day 30, he discharged with daily dental care.
【Discussion】
The antigens of Staphylococcus and Streptococcus are recognized to be important cause of liver abscess followed by Candida, Klebsiella, tuberculosis, Gram negative bacteria and Amebiasis (1-3). Fusobacterium which belongs to the Gram negative bacteria is one of the oral cavity bacteria (2, 3). It causes oto-laryngeal infection, pharyngeal and para-nasal cavity infection, pleural empyema, postoperative infection and liver abscess (2, 3). Of the previously reported twelve cases with liver abscess caused by fusobacterium, five cases owned single nodule and seven cases, multiple nodules (2). In our case, Fusobacterium from oral cavity inflammation from his unclean teeth caused liver abscess of more than ten nodules and subdural empyema. Then, antibiotics infusion was the first choice instead of hepatic drainage. The optimal antibiotics induced the dramatic shrinkage of the inflammatory focuses.
Cranial subdural empyema is arising most by direct spread from an intracranial
infection but rarely by septic thrombophlebitis (4, 5). The mortality rate is reported to be about 6-35%, and appoximately 55% of patients have neurological deficits at the time of hospital discharge (4). Nathoon N et al. reported that of the 699 cases with intracranial empyema, 6 cases were associated with liver abscess (6). Kojima et al. recently reported a case with liver abscess and subdural empyema caused by Klebsiella which was treated by hepatic and cranial drainages (1).As a management of subdural empyema, surgery is not always the first choice (7).
In our case, it is considered that septicemia first occurs from mild appendicitis or dental inflammation, inducing hematogeneous spread to liver abscess and subdural empyema via septic thrombophlebitis of bridging vein. The early diagnosis and the infusion of the optimal antibiotics led to cure the inflammation and discharge without any morbidity.
【Summary】
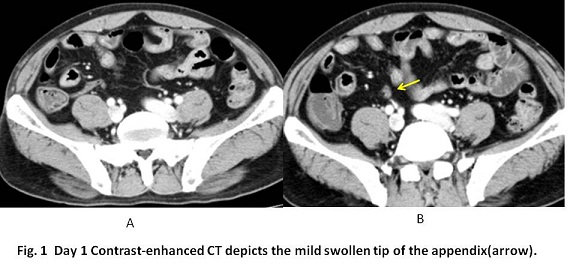
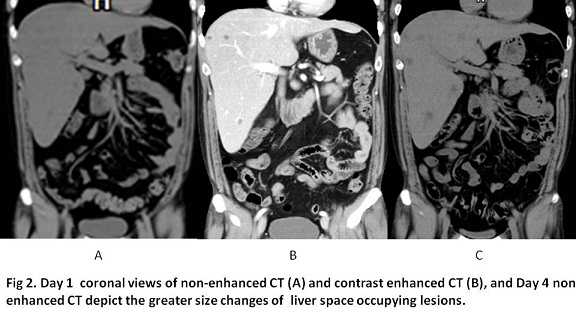
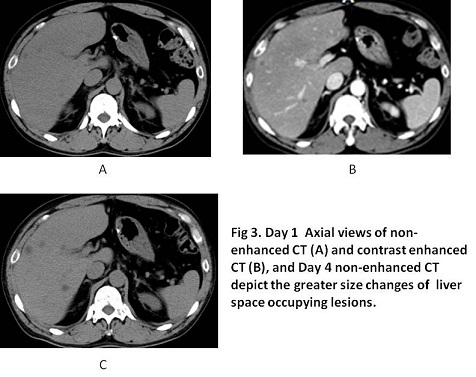
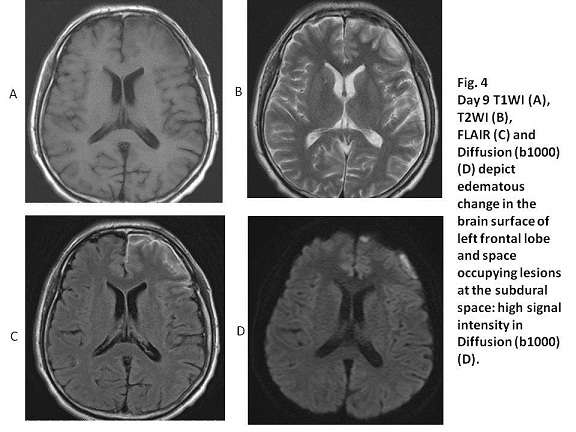
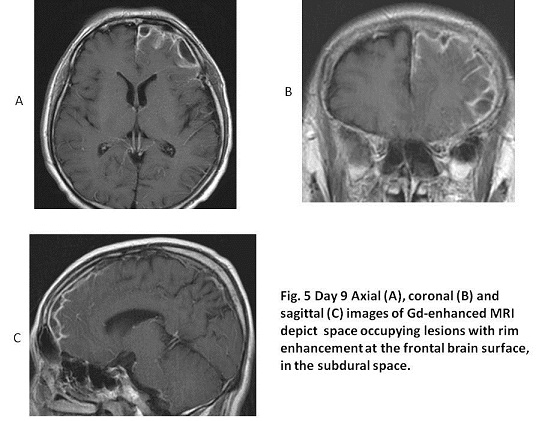
A forty one-year-old male suffering from high fever, abdominal pain and headache, came to our hospital. He did not have a habit to brush teeth regularly and had several decayed teeth. Day 1 and 4 CT depicted the liver abscess with multiple foci. Day 9 Gd-enhanced MRI showed subdural empyema. Fusobacterium was isolated from blood culture and the appropriate antibiotics induced remarkable shrinkage of liver abscess and subdural empyema, leading to discharge without any morbidity.The early diagnosis and the optimal treatment is crucial for overcoming the abscess originated from oral bacteria.
【References】
1.Kojima A, et al. Supra- and infratentorial subdural empyema secondary to septicemia in a patient with liver abscess--case report. Neurol Med Chir 2004;44: 90-93
2.Kawasaki C, et al. Retrospective Analysis of Fusobacterium associated Infections;Experience at Aomori Prefectural Hospital with 108 cases from 1995 to 1999 Kannsennsyo 2002; 76: 23-31 (Japanese).
3.Yoneda M, et al. Liver abscess caused by periodontal bacterial infection with Fusobacterium necrophorum. Hepatology Research 2011; 41: 194―196
4.Dawodu ST, et al. Subdural Empyema: Background, Pathophysiology, Epidemiology 2015; emedicine.medscape.com/article/1168415-overview
5.Wu TJ, et al. Subdural empyema . J Microbiol Immunol Infect 2008; 41: 62–67
6.Nathoon N et al. Intracranial subdural empyema in the era of computed tomography : a review of 699 cases. Neurosurgery 1999; 44:529-536
7.Leys et al. Management of subdural intracranial empyema should not always require surgery. Neural Neurosurg Psychiatry 1986; 49: 635-639
2016.06.15
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.