

Clinical diagnosis
Case 17
The antibiotics were continuously given for the suspicious cholecystitis. The high values of CRP and WBC counts continued but eventually gradually lowered almost to the normal level. As the underlying condition, multiple myeloma was listed because of the high value of IgG and hypercalcemia. The patient still stays for further investigation and treatment.
【Discussion】
Retroperitoneal abscess is known to occur as a secondary complication of infections; osteomyelitis of the lumbar vertebrae (1-3): cold Tbc abscess from lumbar disk, injuries or malignancies of retroperitoneal organs (2). Further, it occurs via suppurative lymphadenitis or bacteremia (1, 3). Diabetes mellitus, previous surgery and an immunosuppressive condition were common underlying conditions (1). Over half of the patients were more than fifty years of age (1). The age of our case was eighty eight years old and she had the suspicious multiple myeloma as the underlying condition and the retroperitoneal abscess was considered to be caused by bacteremia.
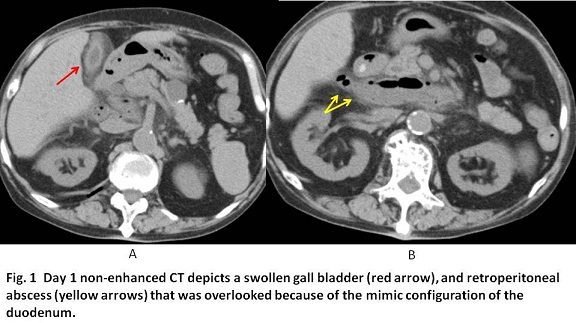
The retroperitoneum is situated between the posterior parietal peritoneum anteriorly and the transversalis fascia posteriorly (4). The retroperitoneum is broadly divided into the anterior and posterior pararenal, perirenal, and great vessel spaces. The anterior pararenal space is bordered anteriorly by the posterior parietal peritoneum, posteriorly by the anterior renal fascia (Gerota fascia), and laterally by the lateroconal fascia. The anterior pararenal space is subdivided into the pancreaticoduodenal subspace, which contains the pancreas and duodenum, and the pericolonic subspace, which contains the ascending and descending colon (4). When pancreatitis occurs, the pancreatic fluids sometimes infiltrate the whole anterior pararenal space. In our case, the retroperitoneal abscess was localized in a part of pancreaticoduodenal subspace of the anterior pararenal space. Namely, the present retroperitoneal abscess situated at the dorsal portion adjacent with the duodenum and then, it was overlooked in Day1 CT because of the mimic configuration of the duodenum. Enhanced CT using contrast medium was not conducted because of the low eGFR value and the multiple myeloma.
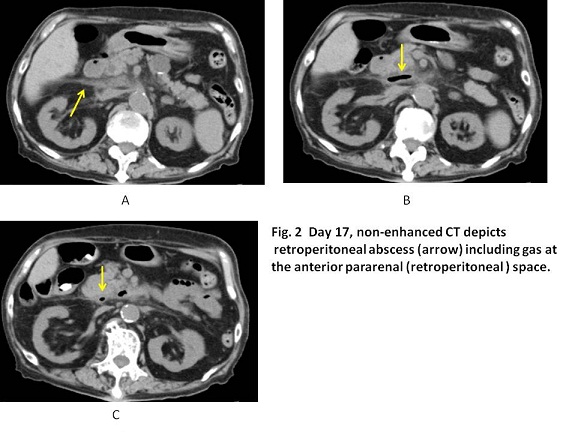
As the management for the retroperitoneal abscess, the pigtail drainage and the surgical drainage are listed (5). As a result, the drainage was not attempted in our case. A recent report said that Escherichia coli was the most prevalent pathogen (31.3%) for retroperitoneal abscess, followed by Klebsiella pneumoniae (25%) (1). The optimal selection for antibiotics is crucial. Fortunately, the continuation infusion of antibiotics led to the disappearance of retroperitoneal abscess in our case.
【Summary】
We encountered an eighty eight female with retroperitoneal abscess. Because of low level of eGFR and the underlying disease of multiple myeloma, contrast-enhanced CT was not performed. The present retroperitoneal abscess situated at the pancreatico-duodenal subspace of the anterior pararenal space, which mimicked the duodenum. Although our case is rare, the detailed interpretation of CT image is crucial with keeping in mind of the presence of the pancreatico-duodenal subspace.
【References】
1.Huang SH, et al. Retroperitoneal abscess: 7-year experience of 29 cases in a tertiary care center in Taiwan Urological Science 2015; 26: 218-221.
2.Altemeier ,WA, et al. Retroperitoneal Abscess. Arch Surg. 1961;83 :512-524. doi:10.1001/archsurg.1961.01300160024004.
3.La Greca G, et al. Retroperitoneal abscess-rare causes and atypical manifestation: report of two cases. Surg Today 1995; 25: 965-969
4.Tirkes T, et al. Perineal and retroperitoneal anatomy and its relevance for cross sectional imaging. RadioGraics 2012; 32: 437-451
5.Crepps JT, et al. Management and outcome of retroperitoneal abscesses. Ann Surg. 1987: 205: 276–281.
2016.8.3
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.