

Clinical diagnosis
Case 18
Our pediatrics introduced this patient to National Pediatric Center for further investigation and consultation about treatment.
【Discussion】
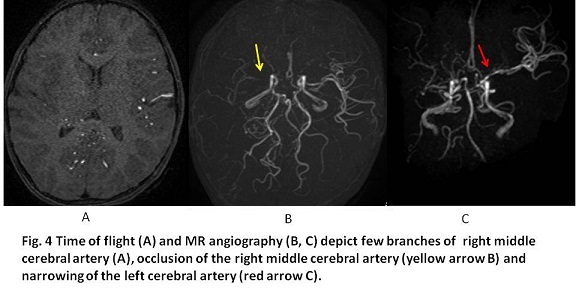
Moyamoya disease (MMD) is an occlusive cerebrovascular disease characterized by the progressive stenosis or occlusion of the distal branch of internal carotid artery, resulting in fine collateral network called moyamoya vessel. Pathological features of the occlusive arteries are primarily thickness of the intima (1). In short, the histopathological findings in the occlusive artery have shown fibrin deposits in the wall, a proliferation of the smooth muscle cells or endothelium, a stenosis or occlusion associated with the fibrocellular thickening of the intima and the formation of microaneurysms (2). In addition, cortical microvascularization, which is characterized by a substantially increased microvascular density and diameter, is suggested as a specific finding in MMD (1, 2). In our case, MRA showed the occlusion of the right middle cerebral artery and a narrowing of the left middle cerebral artery with collaterals from the posterior cerebral artery.
Recently, Ring finger protein (RNF) 213 gene was shown to be strongly associated with MMD occurrence and evaluated as a susceptibility gene for MMD (1, 3). However, the total mechanisms leading from RNF213 mutations to MMD clinical features are still unknown. The addition of environmental factors such as autoimmune or inflammation might be relevant with the determinate occurrence for MMD (1). Our case will be scheduled to take the gene investigation.
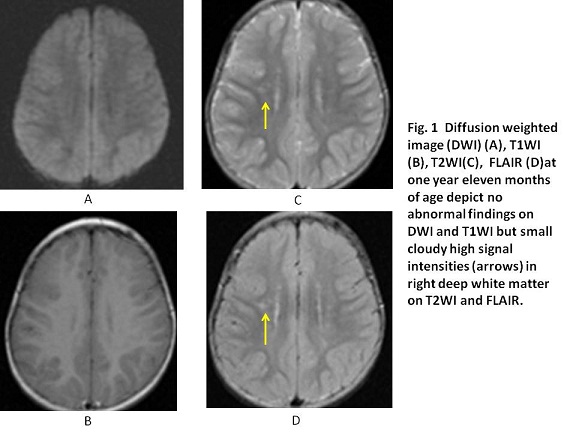
Leptomeningeal high signal intensity (ivy sign) on MRI is reported to appear in which cortical branches of the middle cerebral arteries were poorly visualized on MR angiography (4, 5). In our case, ivy sign was not found but high signal intensity in the deep white matter corresponded to the area of the occlusive left middle cerebral artery.
Radical treatments for MMD do not exist. However, surgical managements for MMD, such as the direct anastomosis of temporal artery-middle cerebral artery bypass, the indirect anastomosis of encephalo-duro-myo-synangiosis and the both combination, are effective (6, 7). The feasibility of the direct anastomosis in children is limited because of the small size of the vessels (7). Indirect techniques might be favored in pediatric patients due to their simplicity and good clinical results (6, 7). The relative cerebral blood flow is reported to be increased by 15.5% from the gradual formation of anastomoses as a result of indirect revascularization (6). In our case, surgical management is not determined because of the mild symptom and young age.
【Summary】
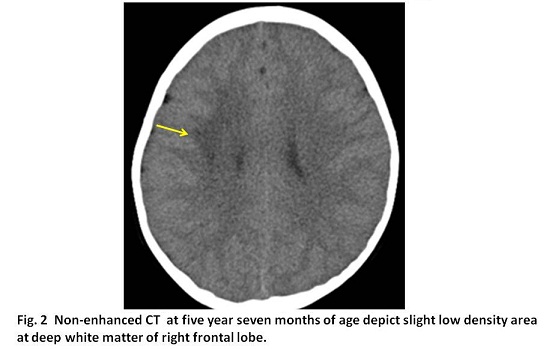
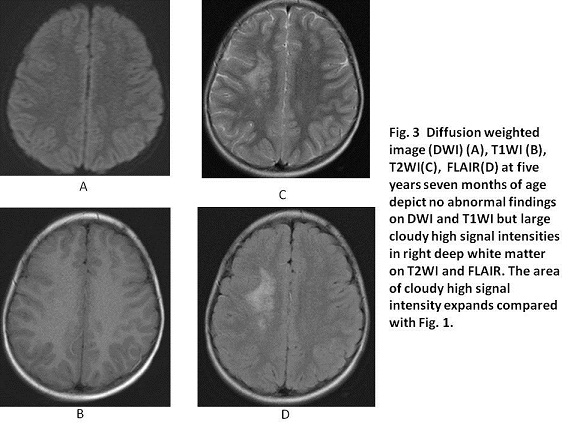
We present a case with MMD at the onset of infant. FLAIR and T2WI of MRI performed at one year seven months and five years seven months showed the high signal intensity at the right-sided deep white matter, enlarging with the age. MRA showed the occlusion of the right middle cerebral artery with the collaterals from the right posterior cerebral artery and the lumen stenosis of the left middle cerebral artery. As the initial MRI finding of MMD, the cloudy high signal intensity at the deep white matter appears,which might be valuable to keep in mind.
【References】
1.Bang OY, et al., The Pathophysiology of Moyamoya Disease: An Update J Stroke. 2016; 18: 12–20. Published online 2016 Jan 29. doi:10.5853/jos.2015.01760
2.Bersano A, et al. Research Progresses in Understanding the Pathophysiology of Moyamoya Disease. Cerebrovasc Dis. 2016;41:105-18. doi: 10.1159/000442298. Epub 2016 Jan 12.
3.Koizumi A, et al. A new horizon of moyamoya disease and associated health risks explored through RNF213. Environ Health Prev Med. 2016;21:55-70. doi: 10.1007/s12199-015-0498-7. Epub 2015 Dec 10.
4.Yoon HK et al. "Ivy sign" in childhood moyamoya disease: depiction on FLAIR and contrast-enhanced T1-weighted MR images. Radiology. 2002;223:384-389.
5.Fujiwara H, et al. Leptomeningeal high signal intensity (ivy sign) on fluid-attenuated inversion-recovery (FLAIR) MR images in moyamoya disease. Eur J Radiol. 2005;55 :224-230. Epub 2004 Dec 28.
6.Xu B, et al. Superficial temporal artery-middle cerebral artery bypass combined with encephalo-duro-myo-synangiosis in treating moyamoya disease: surgical techniques, indications and midterm follow-up results. Chin Med J (Engl). 2012 Dec;125(24):4398-4405
7.Bohara M, et al. Effect of Revascularization on Headache Associated with Moyamoya Disease in Pediatric Patients. Hiroshima J Med Sci. 2015 ;64:39-44.
2016.8.10
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.