

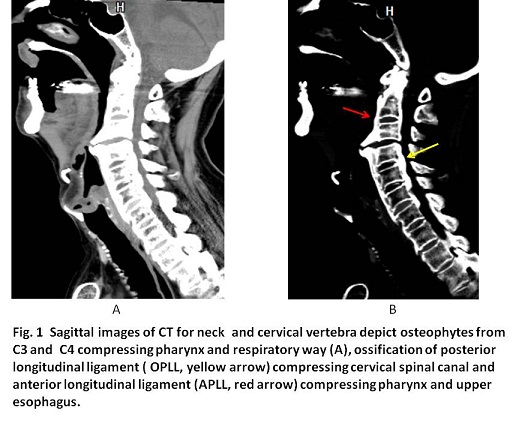
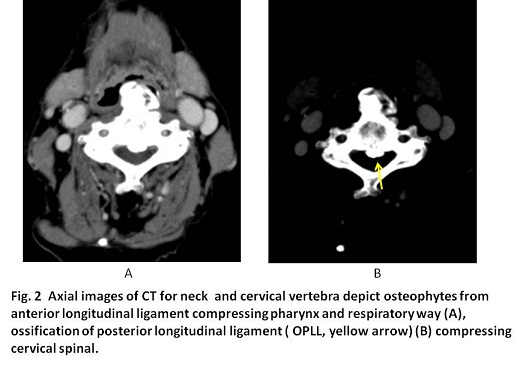
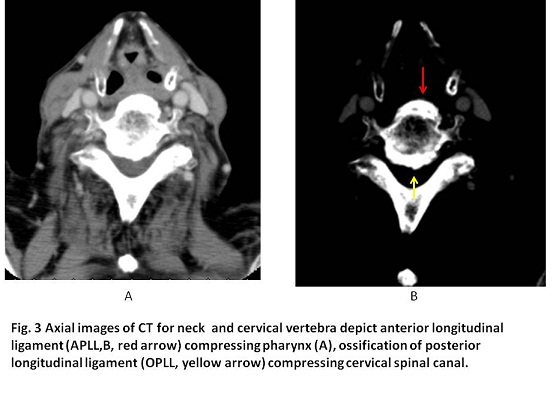
Imaging findings
Case 31
Our anesthetist had once experienced another case with the difficulty of tracheal tube insertion prior to general anesthesia due to the presence of ossification of anterior longitudinal ligament. For this case, the problem might also occur during the procedure of general anesthesia. At present, breathing symptoms were not found. The patient was introduced to the expert orthopedist for spine surgery and scheduled to be given a surgical removal of bony spur at C3 and C4.
【Discussion】
Osteophytes are usually symptomless but cause pain or numbness when they impinge or compress the adjacent nerve. Osteophytes seem to occur at any skeletal bone and result from prolonged wear and tear. Intervertebral disks lose hydration and elasticity with age, and these losses lead to cracks and fissures. The surrounding ligaments also lose their elastic properties and develop traction spurs. However, others argue that the causes of osteophytes are not only the stress but the decrease in reparative abilities with age. Recent studies revealed transforming growth factor β (TGFβ) in case of neovasculization for reparative process, is a crucial factor to induce osteophytes. In short, although the details are not clarified, TGFβ works to turn precursor cells of peiosteum into osteoblastic cells that develope osteophytes. In our patient aged 82, osteopytes developed progressively with age and eventually compress the esophagus. Further, ossifications of anterior longitudinal ligament (APLL) and posterior longitudinal ligament (OPLL) were found. Ossification of APLL is now classified into diffuse idiopathic skeletal hyperostosis (DISH). Pathogenesis of DISH is reported that atherosclerosis of the nutrition artery first ocurrs at the immobination vertebrae and damges to endothelium, inducing the aggregation of platelets and producing platelet –derived growth factor followed by osteoblast proliferation and/or the osteoblastic differentiation of undifferentiated mesenchymal cells in the ligaments (15-18). Ossification of anterior longitudinal ligament of DISH is the least morbidity significance but possible complications described in the literature are dysphagia, stridor, dyspnea and/or myelopathy and hoarseness (19-22). Our patient had osteophytes with marked ossification of anterior longitudinal ligament which is termed DISH.
The incidence of ossification of posterior longitudinal ligament is approximately 2.5 % in Japanese and twice as common in men compared with women. Symptoms usually manifest in forties to sixties. OPLL is often associated with several other entities: DISH, ossification of the yellow ligament (OYL) and ankylosing spondylitis. Stages of spinal cord damage by OPLL are as follows; stage 0 normal or mild compression of anterior horn without neuronal loss; stage 1 mild compression of anterior horn with partial neuronal loss; stage 2 marked deformity of anterior horn; severe neuronal loss :stage 3 severe spinal cord damage. The pathogenesis of OPLL is not fully understood but it is clear that the occurrence of OPLL has a genetic background which is supported by family studies, and twin studies. Our patient owned cervical spondylosis with marked osteopyhtes, APLL and OPLL. The common genetic mechanism of these skeletal change has not yet been identified.
In our case, dysphagia was the main symptom due to compression of marked osteopytes of APLL. He was scheduled to surgical removal: approach from the skin incision along with the anterior edge of sternocleidomasoideus muscle and the excision of the osteophytes mass.
【Summary】
We present an eighty two-year-old patient suffering from the gradual dysphagia due to protrusion of anterior osteophytes mass from vertebras of C3 and C4 accompanied with ossification of anterior and posterior longitudinal ligaments from levels of C1 to C7. These changes are referred as DISH or Forestier’s disease. The pathogenesis of ossification is getting clarified that atherosclerosis of neutrient vessels produces platelet-derived growth factor, inducing osteoblasts activity, transforming undifferentiated mesenchymal cells to osteobalasts differentiation and forming calcification and ossification of ligament. Most patients had less symtoms but the progressively thick ossification with osteophyte mass causes dysphagia such as our patient. The patient was scheduled to surgical removal of the osteophyte mass.
【References】
1.Jiménez-Balderas FJ, Mintz G (1993). "Ankylosing spondylitis: clinical course in women and men". J Rheumatol. 20 (12): 2069–2072
2.Yu DT. Clinical manifestations of ankylosing spondylitis in adults. http://www.uptodate.com/home. Accessed Sept. 12, 2013.
3.Slonimsky E, Pelvic enthesopathy on CT is significantly more prevalent in patients with diffuse idiopathic skeletal hyperostosis (DISH) compared with matched control patients. Clin Rheumatol. 2016 Jul;35(7):1823-7. doi: 10.1007/s10067-015-3151-3. Epub 2015 Dec 21.
4.Forestier J, Rotes–Querol J: Senile ankylosing hyperostosis of the spine. Ann Rheum Dis 1950, 9:321–330.
5.Mader R: Diffuse idiopathic skeletal hyperostosis: a distinct clinical entity. Isr Med Assoc J 2003, 5:506–508. This article provides a clear and definitive definition of DISH as a clinical entity that is distinct from osteoarthrosis on the basis of epidemiologic, pathogenetic, clinical, and radiologic data.
6.Resnick D, Shapiro RF, Wiesner KB, et al.: Diffuse idiopathic skeletal hyperostosis (DISH): ankylosing hyperostosis of Forestier and Rotés Querol. Semin Arthritis Rheum 1978, 7:153–187.
7.Benjamin M, Kumai T, Milz S, et al.: The skeletal attachment of tendons— tendon “entheses.” Comp Biochem Physiol A Mol Integr Physiol 2002, 133:931–945.
8.Resnick D, Niwayama G: Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 1976, 119:559–568. 7 Utsinger PD: Diffuse idiopathic skeletal hyperostosis Clin Rheum Dis 1985, 7:153–187.
9.Ehara S, Shimamura T, Nakamura R, et al.: Paravertebral ligamentous ossification: DISH, OPLL and OLF. Eur J Radiol 1998, 27:196–205.
10.Resnick D, Guerra J, Robinson CA, et al.: Association of diffuse idiopathic skeletal hyperostosis (DISH) and calcification and ossification of the posterior longitudinal ligament. AJR Am J Roentgenol 1978, 131:1049–1053.
11.Hukuda S, Mochizuki T, Ogata M, et al.: The pattern of spinal and extraspinal hyperostosis in patients with ossification of the posterior longitudinal ligament and the ligamentum flavum causing myelopathy. Skeletal Radiol 1983, 10:79–85.
12.Sharma RR, Mahapatra A, Pawar SJ, et al.: Spinal cord and cauda equina compression in ‘DISH.’ Neurol India 2001, 49:148–152.
13.Federici A, Sgadari A, Savo A, et al.: Diffuse idiopathic skeletal hyperostosis: an uncommon case of dysphagia in an older adult. Aging Clin Exp Res 2003, 15:343–346. This case report shows that DISH is not only responsible for the ossification of the anterior longitudinal ligament but, in the elderly, can also give rise to complex clinical pictures that need to be suspected and identified.
14.Ebo D, Goethals L, Bracke P, et al.: Dysphagia in a patient with giant osteophytes: case presentation and review of the literature. Clin Rheumatol 2000, 19:70–72.
15.Kiss C, Szilagyi M, Paksy A, et al.: Risk factors for diffuse idiopathic skeletal hyperostosis: a case–control study. Rheumatology 2002, 41:27–30.
16.Zebboudj AF, Imura M, Bostrom K: Matrix GLA protein, a regulatory protein for bone morphogenetic protein-2. J Biol Chem 2002, 8; 277:4388–4394.
17.Dhore CR, Cleutjens JP, Lutgens E, et al.: Differential expression of bone matrix regulatory proteins in human atherosclerotic plaques. Arterioscler Thromb Vasc Biol 2001, 21:1998–2003.
18.Zebboudj AF, Shin V, Bostrom K, et al.: Matrix GLA protein and BMP-2 regulate osteoinduction in calcifying vascular cells. J Cell Biochem 2003, 90:756–765.
19.Hirano H, Suzuki H, Sakakibara T, et al: Dysphagia due to hypertrophic cervical osteophytes. Clin Orthop. 1982, 167: 168-172
20.Hilding DA, Tachdjian MO: Dysphagia and hypertrophic spurring of the cervical spine. N Engl J Med. 1960, 263: 11-14.
21.Kmucha ST, Cravens RB: DISH syndrome and its role in dysphagia. Otolaryngol Head Neck Surg. 1994, 110 (4): 431-436.
22.Eviatar E, Harel M: Diffuse idiopathic skeletal hyperostosis with dysphagia. J Laryngol Otol. 1987, 101 (6): 627-632. 10.1017/S0022215100102403.
2016.11.9
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.