

Clinical diagnosis
Case 36
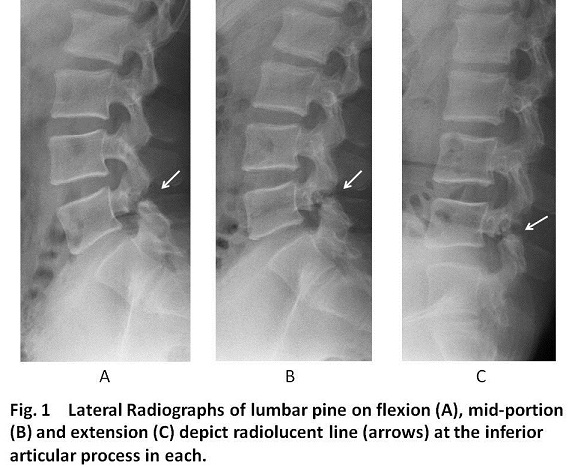
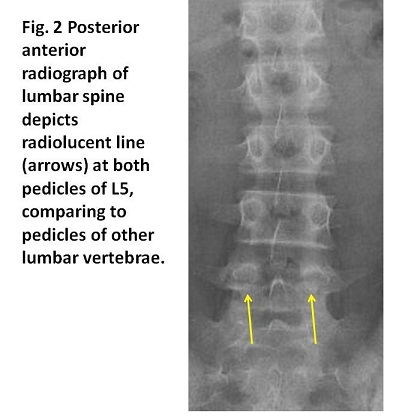
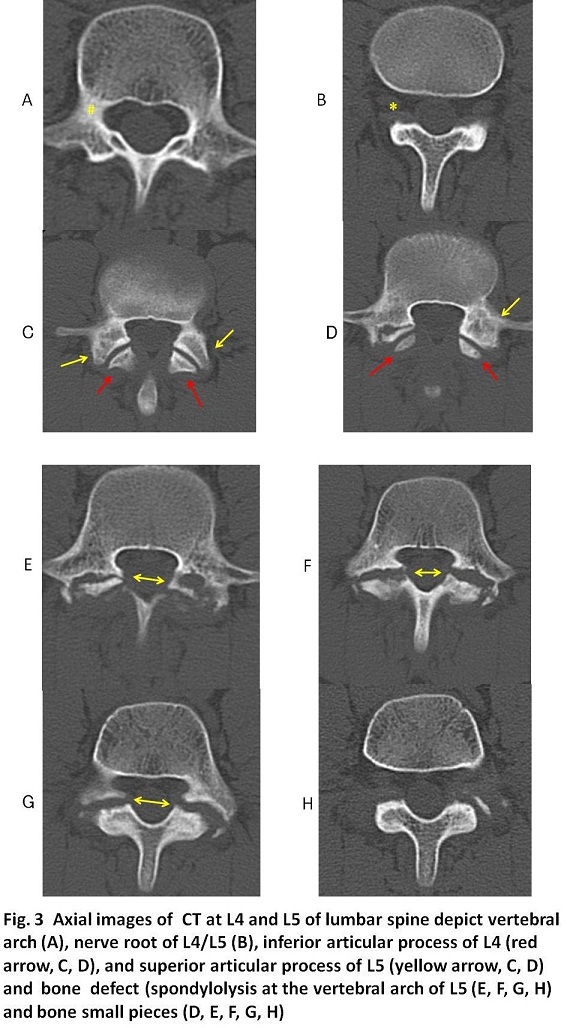
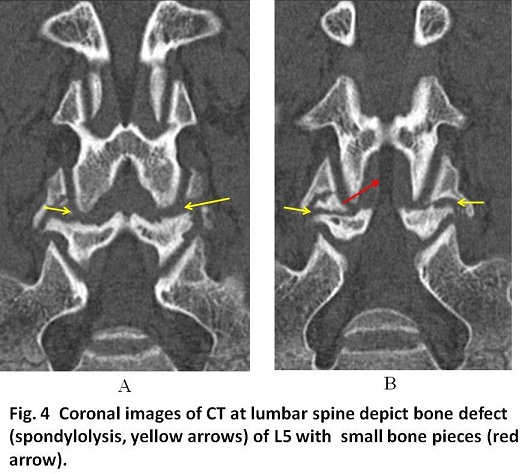
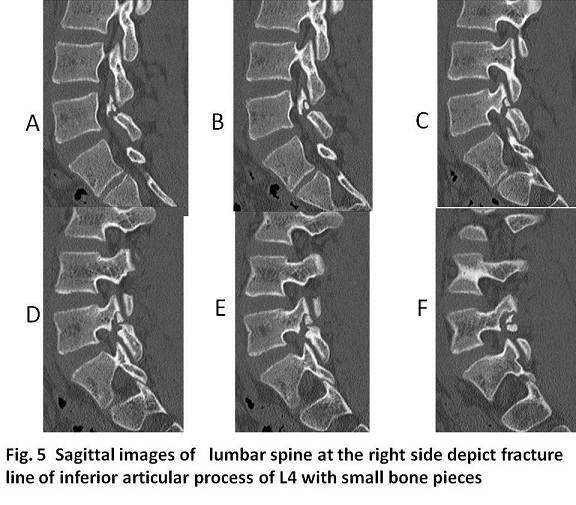
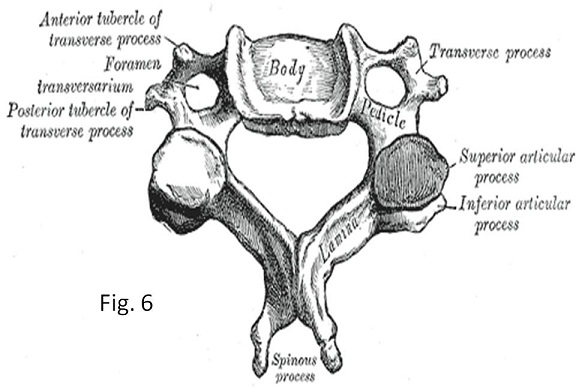
Spondylolysis is one of the common causes of back pain (1). Spondylolysis is a bone defect of the pars interarticularis which is the part of vertebral arch located between the inferior and superior articular processes of the facet joint. The cause of spondylolysis is fatigue fracture and congenital anomaly might be possible with least incidence (1-3). Patients with spina bifida occulta is known to have an increased risk for spondylolysis (4). From the pars interarticularis, the superior articular process extends lateral-upward, while the inferior articular process extends medial-downward. In short, thin piece of pars interarticularis connects the upper and lower segments of the facet joints. The facet joints link the vertebrae directly above and below to form a working unit that permits movement of the spine. In the axial plane, pars interariticularis is the bony mass between the lamina and pedicle. Namely, the bony mass lies anterior to the lamina and posterior to pedicle(Fig.6). When force of flexion (bending forward) is charged, pars interarticularis get pressure from the superior articular process, while when force of extension (bending backward) is charged, pars interarticularis get pressure from the inferior articular process (1). Because in erect posture, the body weight is supported most in the lower lumbar spine, the burden of L5 is the greatest (1-3). Repeated exercises of flexion and extension are predisposed to fatigue fracture of pars interarticularis especially in teens during the bone growing process. Lumbar spondylolysis is most common at L5 with the incidence 85% (1, 5) and it sometimes occur a L5 slip forward termed spondylolisthesis (1-3). In our case, fatigue fracture of pars interarticularis of L4 occurred in a sixteen year-old boy who plays baseball. CT showed bilateral spondylolysis with small bone fragments due to fatigue fracture of bilateral pars articularis. On an anterior oblique radiograph or coronal CT (Fig. 4), pars interarticularis correspond to the neck of the imaginary Scottie dog (1-3); its ear superior articular process, its foreleg inferior articular process, its nose transverse process, its body articular arch overlapping spinous process, its face (or eye) pedicle. Interpretation of axial images on CT is sometimes difficult to differentiate spondylolysis from the normal facet joint. The bone defect image of spondylolysis mimics to the facet joint. In healthy vertebrae, after articular arch is visualized, nerve root foramen is next visualized followed by the facet joint of the inferior articular process of the present vertebrae and superior articular process of the next lower vertebrae. Thereafter, the next vertebral arch is visualized. The repetition of this image cycle is continued on axial CT images. Bone defect of spondylolysis is visualized at the level of articular arch because the pars articularis is a part of the articular arch. The sagittal and coronal CT images are easier to discriminate spondylolysis from the facet joint. In our case, axial CT images showed absence of articular arch of L4, suspicious spondylolysis. Sagittal and coronal CT images easily identified the spondylolysis with small bone pieces rather than axial CT images. When axial images of spondylolysis are encountered, the recognition of the normal cycle above should keep in mind in order not to overlook spondylolysis.
Initial treatment for back pain of spondylolysis is always conservative, prescribing non steroidal anti-inflammatory drug for reduction of pain and healing the fatigue fracture (1-3, 5). The patient is recommended to take break far from taking sports. A brace for back support might be effective to heal the small fatigue fracture and fusion of the pars interarticularis (1-3 5, 6). In case of large fracture such as our case, the fusion might be difficult irrespective of use of brace. If NSAIDs do not provide relief, stronger medication might be prescribed. A rehabilitation program for strengthen muscles stabling lumbar spine will help increase pain-free movement (6).
【Summary】
We present a sixteen year-old boy suffering from lower back pain. Radiograph and lumbar CT showed bone defect of pars articularis of L4. On CT axial image interpretation for lumbar spondylolysis, you should keep in mind that in healthy vertebra, repetition cycle images of vertebral arch, lumbar nerve root foramen and facet joint of superior articular process and inferior articular process and that superior articular process extend upper and a little outer-ward and inferior articular process extend inferior and a little medial-ward. Further, bone defect of pars interarticularis for spondylolysis visualized at the level of vertebral arch of L4 or L5
【References】
1.WebMD (2009). "spondylolysis". Webster's New World Medical Dictionary (3rd ed.). Houghton Mifflin Harcourt. p. 399. ISBN 978-0-544-18897-6
2.Sakai T, et al. Incidence and etiology of lumbar spondylolysis: review of the literature. J Orthop Sci. 2010;15:281–288. [PubMed]
3.Nathan H. Spondylolysis; its anatomy and mechanism of development. J Bone Joint Surg Am.1959;41:303–20. [PubMed]
4.Tanaka Y, et al. Atypical lumbar spondylolysis causing cauda equine syndrome; a report of two cases. Tohoku Arch Orthop Surg Traumatol. 1998;42:181–184. in Japanese.
5.Koakutsu T, et al. Bilateral spondylolysis of inferior articular processes of the fourth lumbar vertebra: a case report Ups J Med Sci. 2012 Mar; 117(1): 72–77. Published online 2012 Feb 15. doi: 10.3109/03009734.2011.629750
6.Physical Medicine and Rehabilitation for Stress Fractures at eMedicine
2016.12.14
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.