

Clinical diagnosis
Case 39
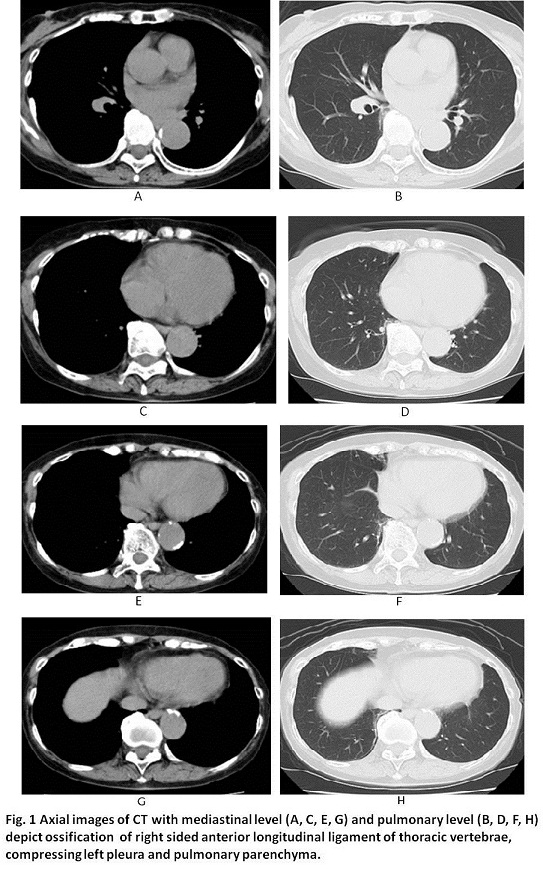
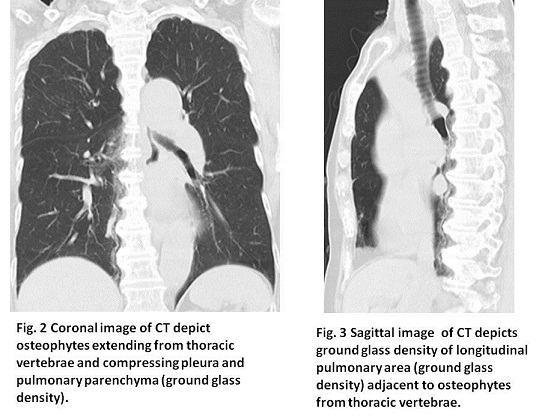
All clinical data was openly shown to the patient. There were no responsible findings except osteophytes of thoracic vertebrae compressing pleura and pulmonary parenchyma. She was given analgesics and anti-inflammatory compress tape for local pain relief.
【Discussion】
In the clinical reality, lumbar vertebral osteophytes of degenerative spondylitis are commonly encountered but thoracic vertebral osteophytes are not well-known. The major skeletal bony diseases are listed as follows: degenerative spondylitis, ankylosing spondylitis and diffuse idiopathic skeletal hypersostosis (DISH, Forestier’s disease). Ankylosing spondylitis mainly occurs in lumbar spine (vertebrae forcet, vertebrae margin), sacro-iliac joint and peripheral joint. The occurrence age was the prime age (fourties to fifties) of manhood (1, 2). Pathogenesis of ankylosing spondylitis is considered that inflammation of the marginal ligament, muscle end and/or cartilage of the joint initially happens and then, the replacement of fibrous cartilage and subcartilage bone was followed into granulation tissue and ossification (2).
Meanwhile, DISH is known to be found not only in mammals such as human, monkeys, gorillas, bears, horses and whales but also in dinosaurs. It usually occurs in 15-25% of aged persons (3-5). DISH rarely occurs in patients with younger than 50 years-old but usually occurs with older than 65 years-old, with an increased incidence in patients with obesity, gout and diabetes and with a male: female ratio of 2:1 (4, 5). Unlike ankylosing spondylitis, DISH does not involve the sacroiliac joint (6-9). DISH is characterized by ossification of the anterior longitudinal ligament of the spine and various extraspinal ligaments (5-8). DISH affects the thoracic spine, especially on the right side of anterior longitudinal ligament (9-14). It is considered that the left side of the thoracic vertebrae was mobile because of the heart and thoracic aorta beats (9-14). Exercise is believed to prevent the worsening of atherosclerosis. Pathogenesis of DISH is reported that atherosclerosis of the nutrition artery first occurs at the immobility vertebrae and damages to endothelium of the vessel, inducing the aggregation of platelets and producing platelet –derived growth factor followed by osteoblast proliferation and/or the osteoblastic differentiation of undifferentiated mesenchymal cells in the ligament (15-18). Our patient was a seventy two-year-old female, and had anterolateral ossification of lower thoracic vertebrae which is characteristic of DISH.
DISH is diagnosed based on the Resnick and Niwayama criteria (8); calcifications and ossification along the anterolateral aspect of at least 4 contiguous vertebral bodies, with or without osteophytes; preservation of intervertebral disk height in the involved areas and an absence of excessive disk disease: absence of bony ankylosis of facet joints and absence of sacroiliac erosion, sclerosis or bony fusion. Further, prominent pelvic and greater trochanter osteophytes might have strong discriminating factors between DISH and non-DISH (3). Although we did not have any imaging data on pelvic bone, our patient had the anterior-right lateral ossification of more than 4 thoracic vertebrae which meet the definition of DISH. Ossification of anterior longitudinal ligament and osteophytes of DISH are the least morbidity significance (19-22). However, back pain is the possible complication such as our case.
【Summary】
We present a seventy two-year-old female suffering from chronic right back pain. CT showed ossification of anterior-right lateral longitudinal ossification along with more than 4 lower thoracic vertebrae which meet the definition of DISH. We should keep in mind that DISH occurs at the right anterior aspects of thoracic vertebrae of the aged patients and DISH might be the possible cause of right back pain.
【References】
1.Jiménez-Balderas FJ, Mintz G (1993). "Ankylosing spondylitis: clinical course in women and men". J Rheumatol. 20 (12): 2069–2072
2.Yu DT. Clinical manifestations of ankylosing spondylitis in adults. http://www.uptodate.com/home. Accessed Sept. 12, 2013.
3.Slonimsky E, Pelvic enthesopathy on CT is significantly more prevalent in patients with diffuse idiopathic skeletal hyperostosis (DISH) compared with matched control patients. Clin Rheumatol. 2016 Jul;35(7):1823-7. doi: 10.1007/s10067-015-3151-3. Epub 2015 Dec 21.
4.Forestier J, Rotes–Querol J: Senile ankylosing hyperostosis of the spine. Ann Rheum Dis 1950, 9:321–330.
5.Mader R: Diffuse idiopathic skeletal hyperostosis: a distinct clinical entity. Isr Med Assoc J 2003, 5:506–508. This article provides a clear and definitive definition of DISH as a clinical entity that is distinct from osteoarthrosis on the basis of epidemiologic, pathogenetic, clinical, and radiologic data.
6.Resnick D, Shapiro RF, Wiesner KB, et al.: Diffuse idiopathic skeletal hyperostosis (DISH): ankylosing hyperostosis of Forestier and Rotés Querol. Semin Arthritis Rheum 1978, 7:153–187.
7.Benjamin M, Kumai T, Milz S, et al.: The skeletal attachment of tendons— tendon “entheses.” Comp Biochem Physiol A Mol Integr Physiol 2002, 133:931–945.
8.Resnick D, Niwayama G: Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 1976, 119:559–568. 7 Utsinger PD: Diffuse idiopathic skeletal hyperostosis Clin Rheum Dis 1985, 7:153–187.
9.Ehara S, Shimamura T, Nakamura R, et al.: Paravertebral ligamentous ossification: DISH, OPLL and OLF. Eur J Radiol 1998, 27:196–205.
10.Resnick D, Guerra J, Robinson CA, et al.: Association of diffuse idiopathic skeletal hyperostosis (DISH) and calcification and ossification of the posterior longitudinal ligament. AJR Am J Roentgenol 1978, 131:1049–1053.
11.Hukuda S, Mochizuki T, Ogata M, et al.: The pattern of spinal and extraspinal hyperostosis in patients with ossification of the posterior longitudinal ligament and the ligamentum flavum causing myelopathy. Skeletal Radiol 1983, 10:79–85.
12.Sharma RR, Mahapatra A, Pawar SJ, et al.: Spinal cord and cauda equina compression in ‘DISH.’ Neurol India 2001, 49:148–152.
13.Federici A, Sgadari A, Savo A, et al.: Diffuse idiopathic skeletal hyperostosis: an uncommon case of dysphagia in an older adult. Aging Clin Exp Res 2003, 15:343–346. This case report shows that DISH is not only responsible for the ossification of the anterior longitudinal ligament but, in the elderly, can also give rise to complex clinical pictures that need to be suspected and identified.
14.Ebo D, Goethals L, Bracke P, et al.: Dysphagia in a patient with giant osteophytes: case presentation and review of the literature. Clin Rheumatol 2000, 19:70–72.
15.Kiss C, Szilagyi M, Paksy A, et al.: Risk factors for diffuse idiopathic skeletal hyperostosis: a case–control study. Rheumatology 2002, 41:27–30.
16.Zebboudj AF, Imura M, Bostrom K: Matrix GLA protein, a regulatory protein for bone morphogenetic protein-2. J Biol Chem 2002, 8; 277:4388–4394.
17.Dhore CR, Cleutjens JP, Lutgens E, et al.: Differential expression of bone matrix regulatory proteins in human atherosclerotic plaques. Arterioscler Thromb Vasc Biol 2001, 21:1998–2003.
18.Zebboudj AF, Shin V, Bostrom K, et al.: Matrix GLA protein and BMP-2 regulate osteoinduction in calcifying vascular cells. J Cell Biochem 2003, 90:756–765.
19.Hirano H, Suzuki H, Sakakibara T, et al: Dysphagia due to hypertrophic cervical osteophytes. Clin Orthop. 1982, 167: 168-172.
20.Hilding DA, Tachdjian MO: Dysphagia and hypertrophic spurring of the cervical spine. N Engl J Med. 1960, 263: 11-14.
21.Kmucha ST, Cravens RB: DISH syndrome and its role in dysphagia. Otolaryngol Head Neck Surg. 1994, 110 (4): 431-436.
22.Eviatar E, Harel M: Diffuse idiopathic skeletal hyperostosis with dysphagia. J Laryngol Otol. 1987, 101 (6): 627-632. 10.1017/S0022215100102403.
2017.1.11
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.