

Clinical diagnosis
Case 41
He was given non-steroid anti-inflammatory drug and hospital admission, scheduled for head halting traction followed by soft collar for 4–6 weeks.
【Discussion】
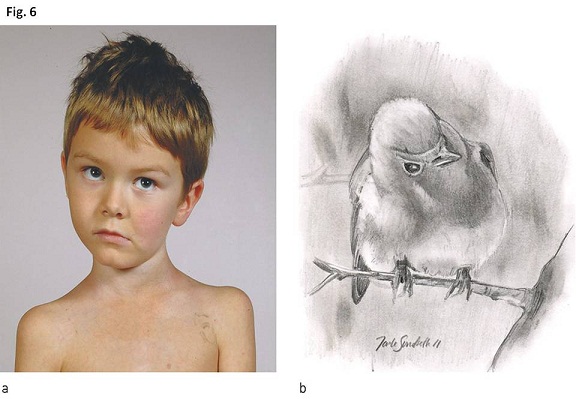
Torticollis is termed when the head of the patient is tilled over to one side (Fig.6) Atlantoaxial rotatory fixation gives rise to torticollis for the most part in children. Both terms of atlantoaxial subluxation and atlantoaxial rotatory fixation are used to describe. Atlantoaxial subluxiation includes chronic types which is caused by rheumatoid arthritis Down syndrome, minor trauma and congenital (1-4). When it occurs in children, acute or subacute atlantoaxial subluxation is often used to term. Chronic atlantoaxial subluxation is defined when the duration of torticollis excess over 2 months (2). Meanwhile, it is known as Grisel syndrome that neck tilting is caused by relaxation of the transverse ligament of the atlanto-axial joint (5). Our patient had tilled his head to left side since he got painful swollen parotid gland due to mumps 40 days ago.
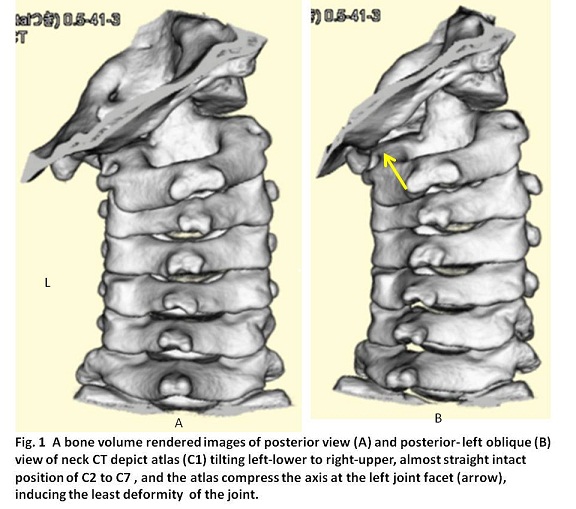
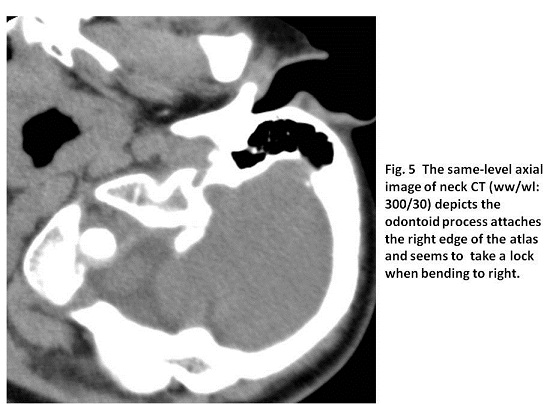
The cause of acute atlantoaxial subluxation is not fully understood. The atlantoaxial joint is stabilized by the odontoid process, which prevents over-deflexion, the transverse ligament which prevents over-flexion, and the alar ligaments which prevent over-rotation (6). In children, a combination of high elasticity of the ligaments and more horizontally oriented facet joints might be the predisposing factors (1, 6). Children have a more convex upper joint surface of the axis which arculates with the lower concave joint surface of the atlas. Further, the head is larger compared to the neck than in adults, and the muscles for supporting head is not well developed (1-4). A combination of these factors is contributing to the high occurrence in children. Once dislocation between joint facet of atlas and axis occurs, it is possibly difficult to be unlocked because of the bony friction. Ishii et al reported that the facet deformity of contact joints between atlas and axis is observed with time progress and the lateral inclination of the atlas gradually increases accompanied with facet depression (7). In our case, volume rendered image of CT depict subluxation with bony friction (Fig.1) which indicates the difficulty of unlock.
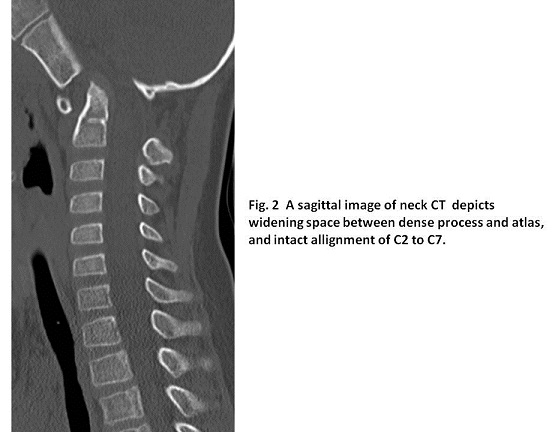
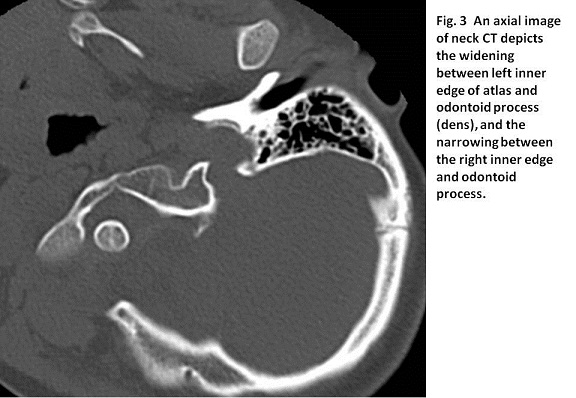
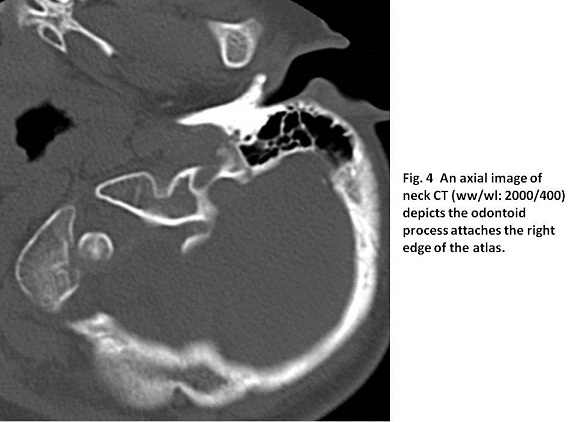
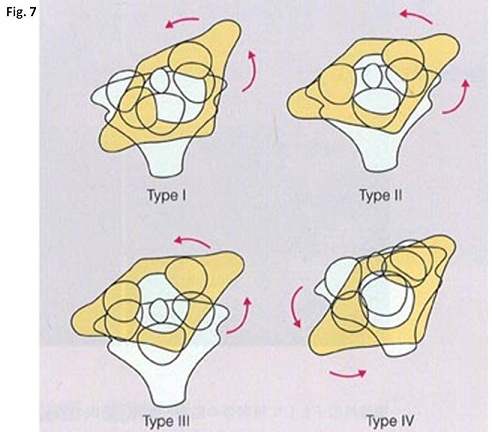
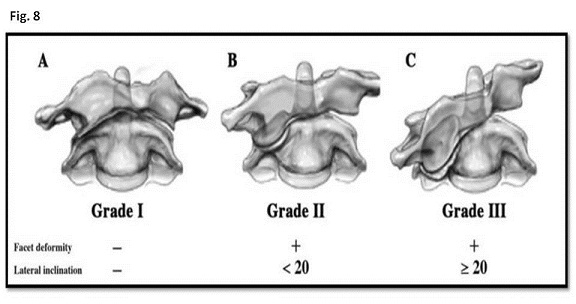
According to the type of the degree of rotatory subluxation, atlantoaxial rotator fixation is categorized in four types (7, 8) ; Type I the atlas is rotated on the dense with no anterior displacement; Type II the atlas is rotated on hemilateral articular process with 3 to 5 mm of anterior displacement; Type III the atlas is rotated on bilateral articular processes with anterior displacement 5 mm or greater: Type IV the atlas rotates and displaces backwards(Fig.7). Atlanto-axial distance is known to be 3 mm or less in adults and 5 mm or less in children (2, 7, 8). Our case whose atolanto-axial distance was 5.6 mm was characterized Type III atlantoaxial rotator fixation. Further, as atlas is usually tilting and the persistent tilting induces the deformity of the facet joint, Ishii K et al. proposed to measure the angle of the tip of bilateral transverse processes of C1 and C2 and the grading of tilting of atlas; Grade I no deformity of the facet; Grade II the facet deformity with slight lateral inclination of less than 20°: the facet deformity with lateral inclination of 20° or more (7, 9)(Fig.8). Our case whose tilting angle is less than 20° with no evidence of the deformity of the joint facet (Fig. 1) is characterized Grade I.
Treatment is decided based on duration of neck tilting (2, 9, 10). In case of neck tilting of 1 week or less duration, NSAIDS and neck collar are given. In case of more than 1 week but l month or less, head halter traction therapy and neck collar for 4 – 6 weeks are given. In case of more than 1 month but less than 3 months, head halter traction for 3 weeks with gradual increase weight and neck vest immobilization for 6 weeks. In case of more than 3 months with neural disorder or failure of previous treatments, C1 and C2 open reduction and arthrodesis are conducted with screws and wiring (2, 9, 10) . In our case, the duration of neck tilting was 40 days at best and then, under hospital admission, head halting traction and neck collar immobilization for several weeks are scheduled.
【Summary】
We present a case of atlantoaxial rotatory fixation whose duration of neck inclination was 40 days. Neck CT showed subluxation of the left joint facet between atlas and axis, atlantoaxial distance of 5.6 mm and tilting angle of atlas of less than 20° but not accompanied with deformity of the subluxation facet. That indicated Type III category and Grade 1 tilting. The duration time was 40 days and then, he underwent head halting traction under hospital admission and neck collar for immobilization for several weeks.
We should keep in mind that the normal distance of atlanto-axial distance is less than 5 mm in children and the normal angle of the tip of bilateral transverse processes of C1 and C2 is horizontal. Further, the earlier duration of atlantoaxial rotatory fixation induces the less invasive treatment.
【References】
1.Ballock RT, Song KM. The prevalence of nonmuscular causes of torticollis in children. J Pediatr Orthop 1996; 16: 500 – 4. [PubMed] [CrossRef]
2.Yang SY. Review of the Diagnosis and Treatment of Atlantoaxial Dislocations. Global Spine J. 2014 Aug; 4(3): 197–210. Published online 2014 May 22. doi: 10.1055/s-0034-1376371
3.Muñiz AE, Belfer RA. Atlantoaxial rotary subluxation in children. Pediatr Emerg Care 1999; 15: 25 – 9. [PubMed] [CrossRef]
4.Sobolewski BA, Mittiga MR, Reed JL. Atlantoaxial rotary subluxation after minor trauma. Pediatr Emerg Care 2008; 24: 852 – 856. [PubMed] [CrossRef]
5.Fernández Cornejo VJ, Martínez-Lage JF, Piqueras C et al. Inflammatory atlanto-axial subluxation (Grisel’s syndrome) in children: clinical diagnosis and management. Childs Nerv Syst 2003; 19: 342 – 347. [PubMed] [CrossRef]
6.Bogduk N, Mercer S. Biomechanics of the cervical spine. I: Normal kinematics. Clinical biomechanics. Nov 2000;15:633-648.
7.Ishii K, Chiba K, Maruiwa H, Nakamura M, Matsumoto M, Toyama Y. Pathognomonic radiological signs for predicting prognosis in patients with chronic atlantoaxial rotatory fixation. Journal of neurosurgery. Spine. Nov 2006;5:385-391.
8.Wortzman G, Dewar FP. Rotary fixation of the atlantoaxial joint: rotational atlantoaxial subluxation. Radiology 1968; 90: 479 – 487. [PubMed]
9.Ishii K, Toyama Y, Nakamura M et al. Management of chronic atlantoaxial rotatory fixation. Spine 2012; 37: E278 – 85
10.Subach BR, McLaughlin MR, Albright AL et al. Current management of pediatric atlantoaxial rotatory subluxation. Spine 1998; 23: 2174 –217 9. [PubMed] [CrossRef]
2017.1.25
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.