

Image findings
Case 42
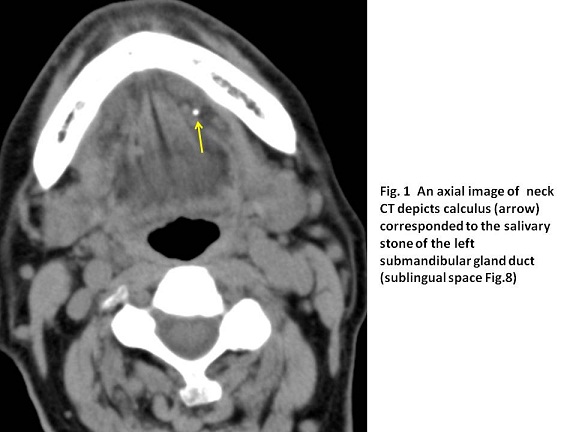
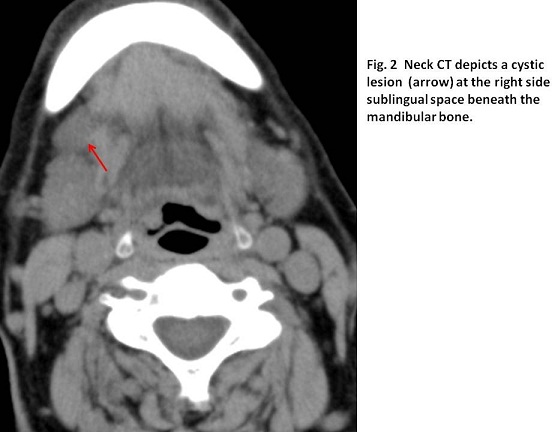
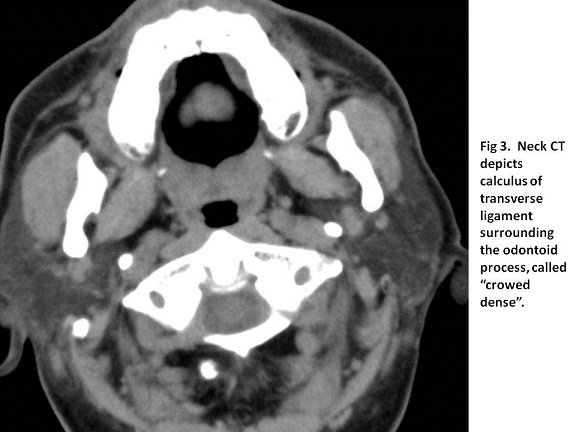
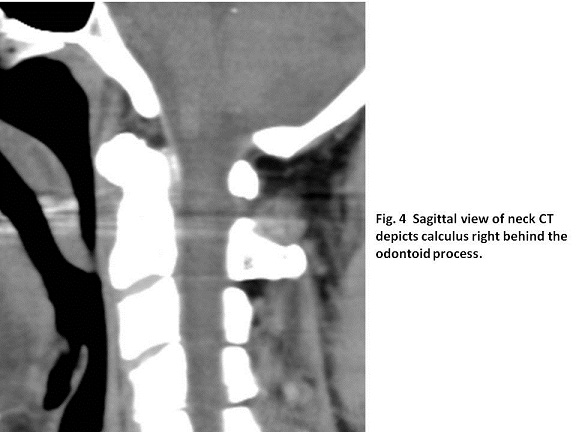
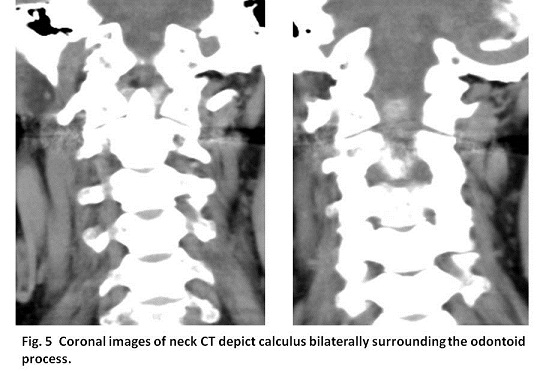
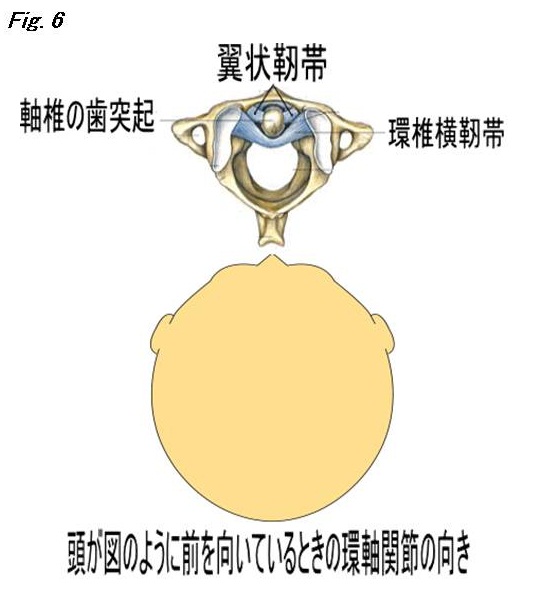
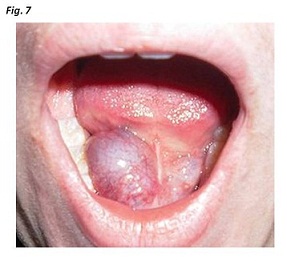
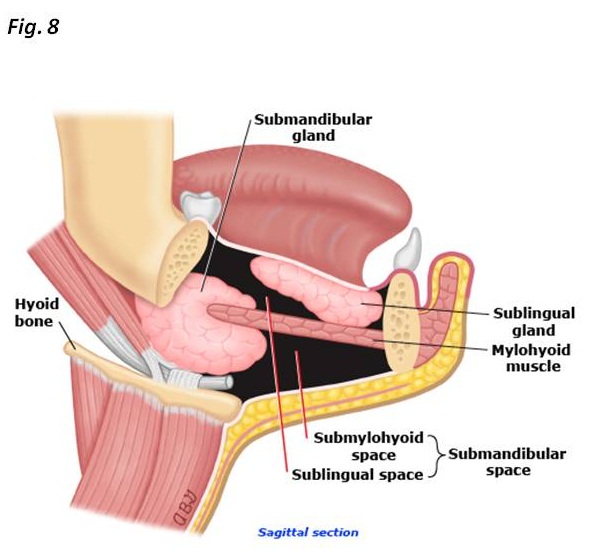
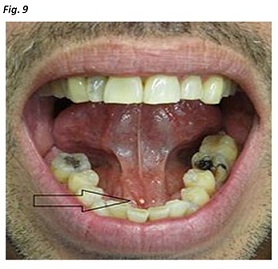
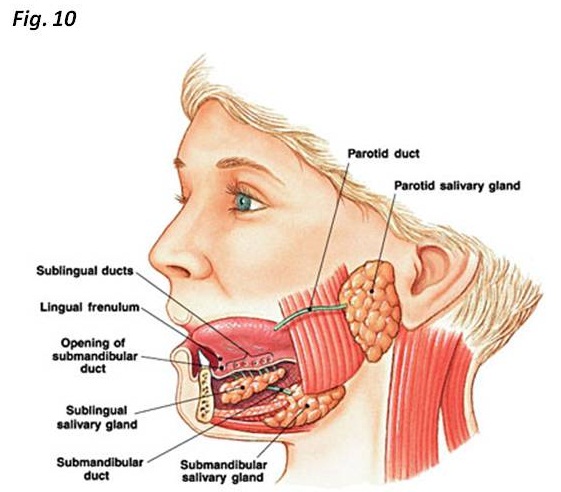
Image findings were explained directly to the patient. As image findings did not show malignancies and reflect his symptoms, he convinced with our explanation and was not given any medicine.
【Discussion】
Crowned dens syndrome with calculus on the transverse ligament (Fig.3,6) was reported to encounter with 5 % incidence of the patients with neck pain over the age of 70 years (1). The calculus is possibly absorbed for a long term follow-up (2). Pathophysiological mechanism of producing the calculus on the transverse ligament and/or alar ligament is not clearly proven. One theory is that chondroid cells which can be found in fibrous cartilage structure in the transverse ligament produce calculus, inducing neck pain (2-4). Another theory is that fibroblasts in the transverse ligament transforms into chondrocytes causing calculus and inducing the symptoms (2-4)(Figs3-6). The calculus crystal is known to be calcium phosphate dehydrate or hydroxyapatite (2). Crowned dense syndrome is defined as an active inflammatory condition resulting from curvelinear calculus surrounding the odontoid process. It typically combined with neck pain and inflammatory markers such as CRP and /or white blood cells (1-7). It is suggested that unless inflammatory symptoms are present, the term of crowned dense syndrome should not be used. In our case, although neck CT showed the typical curvelinear calculus surrounding the odontoid process, the symptom was the feeling of discomfort and laboratory test revealed no elevation of inflammatory markers. Therefore, our case should not be included crown dense syndrome but only periodontoid calculus. However, in the past, our patient might have experienced neck pain accompanied with fresh linear calculus surrounding the odontoid process and resolved spontaneously. The ground of post inflammatory disappearance of calculus is considered not to be convincing because the theory of production and absorbance of calculus is not fully clarified (2).
As the treatment, non-steroid anti-inflammatory drugs are usually used as first-line therapy (1-7). In case without improvement, small doses of corticosteroid are recommended (2). In our case, the symptom was the discomfort feeling of the neck and neck CT showed not merely calculus of the transverse ligament but also sblingular ranula and salivary stone. The responsible cause of the neck discomfort was not clear and no medicine was prescribed.
Ranula is a benign retention cyst (Fig.7) that occurs at the floor of mouth and is categorized based on its extent: simple ranula that is limited to the sublingular space: cervical ranula that is extended into the submandibular (submylohyoid muscle) space(Fig.8)(8,9). Pathological findings revealed ranulas have no epithelial lining and are only pseudocysts surrounded by a condense connective tissue (9). They are probably formed by the leakage of salivary secretions due to inflammation or trauma, inducing to become a thin-walled unilocular homogeneous cystic lesion (10, 11). In our case, CT showed a simple cyst at the sublingular space.
The symptoms of salivary stone are pain and swelling depending on the pressure of the salivary gland, namely completely or partial (Fig.9). When salivary gland is stimulated especially during meal ingestion, the symptoms are manifested which is then, sometimes termed “meal time syndrome”. The cause of salivary gland is unknown but may worse in the presence of chronic inflammation, dehydration or Sjogren’s syndrome. A retrograde theory of forming salivary stone is also possible: food debris might enter the ducts and become nucleus of the stone.
Symptomatic salivary stone occurs with incidence of an approximate half of diseases of major salivary glands and about 0.45 % of the general population (12). It occurs in adults and rarely in children. Salivary stones are found in the submandibular gland with the incidence of 85%, parotid gland with that of 5-10% and others with that of 0-5% (12). The submandibular gland is long and owns two bends; the first at the border of the mylohyoid muscle: the second near the duct orifice (Fig.10). This anatomical factor might cause stasis of saliva, inducing the formation of salivary stone (12-15). Salivary stones which are usually calcium phosphate and calcium carbonate, are not visible on a radiograph in 15-20 % of the cases (14, 15). In our case, salivary stone was small which caused no inflammation and undetectable in radiograph but detected in CT. No treatment was needed.
【Summary】
We present an eighty-year-old male with discomfort of the neck. Neck CT showed sublingular ranula, salivary stone and periodntoid calculus. These imaging findings are not related to his symptoms. However, we should keep in mind that calculus of calcium phosphate of the transverse ligament might cause crowned dens syndrome, that ranula is the retention cyst which appears in the sublingular space and that salivary gland stone which is calcium phosphate or calcium cabonate occurs most in the submandibular gland because it owns long and bending at two sites of mylohyoid muscle and the orifice, inducing the delay of the saliva flow.
【References】
1.Goto S, Umehara J, Aizawa T, Kokubun S. Crowned dens syndrome. J. Bone Joint Surg. Am. 2007; 89: 2732–6.
2.Lee GS, Kim RS, Park HK et al. Crowned dens syndrome: A case report and review of the literature. Korean J. Spine 2014; 11: 15–7.
3.Yamada T, et al. Crowned dens syndrome. Acute Medicine & Surgery 2015; 2: 273
4.Constantin A, Bouteiller G. Acute neck pain and fever as the first manifestation of chondrocalcinosis with calcification of the transverse ligament of the atlas. Five case-reports with a literature review. Rev. Rhum. Engl. Ed 1998; 65: 583–5.
5.Takahashi T, et al. A rare case of crowned dens syndrome mimicking aseptic meningitis. Case Rep. Neurol. 2013; 5: 40–6.
6.Aouba A, Vuillemin-Bodaghi V, Mutschler C et-al. Crowned dens syndrome misdiagnosed as polymyalgia rheumatica, giant cell arteritis, meningitis or spondylitis: an analysis of eight cases. Rheumatology (Oxford). 2004;43 (12): 1508-12. doi:10.1093/rheumatology/keh370 - Pubmed citation
7.Bouvet JP, et al. Acute neck pain due to calcifications surrounding the odontoid process: the crowned dens syndrome. Arthritis Rheum. 1986;28 (12): 1417-20. Pubmed citation
8.Dähnert W. Radiology Review Manual. Lippincott Williams & Wilkins. (2007) ISBN:0781766206. Read it at Google Books
9.Parekh D, Stewart M, Joseph C et-al. Plunging ranula: a report of three cases and review of the literature. Br J Surg. 1987;74 (4): 307-9. Pubmed citation
10.Coit WE, Harnsberger HR, Osborn AG et-al. Ranulas and their mimics: CT evaluation. Radiology. 1987;163 (1): 211-6. Radiology (abstract) - Pubmed citation
11.Kurabayashi T, Ida M, Yasumoto M et-al. MRI of ranulas. Neuroradiology. 2000;42 (12): 917-22. Neuroradiology (link) - Pubmed citation
12.Neville BW, Damm DD, Allen CA, Bouquot JE (2002). Oral & maxillofacial pathology (2nd ed.). Philadelphia: W.B. Saunders. pp. 393–395.
13.Rice, DH (February 1984). "Advances in diagnosis and management of salivary gland diseases.". The Western journal of medicine. 140 (2): 238–49. PMC 1021605 . PMID 6328773
14.Capaccio, P; Torretta, S; Ottavian, F; Sambataro, G; Pignataro, L (August 2007). "Modern management of obstructive salivary diseases.". Acta Otorhinolaryngologica Italica. 27 (4): 161–72. PMC 2640028 . PMID
15.Hupp JR, Ellis E, Tucker MR (2008). Contemporary oral and maxillofacial surgery (5th ed.). St. Louis, Mo.: Mosby Elsevier. pp. 398, 407–409. ISBN 9780323049030.
2017.2.1
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.