

Clinical diagnosis
Case 45

He was recommended to stop running and have a rest for a while until pain abates.
【Discussion】
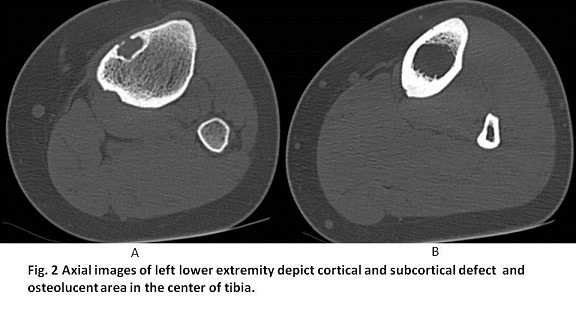
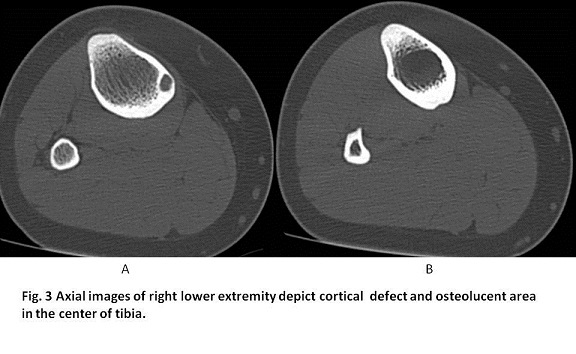
It is reported that nonossifying fibromas are present in approximately 30% of children (1-4). Nonossifying fibroma is considered to be a developmental defect and found in long tubular bone, especially tibia (43%) and femur (38%) in the patients whose ages are less than 20 years (1-4). The lesions are usually osteolucent or osteolytic and occur in the mataphysis or metadiaphysis. They are called fibrous cortical defects when the sizes are less than 2cm in diameter and nonossifying fibroma when they are 2cm or greater (1-3). The latter often expand into meddulary cavity. Histologically, osteolytic lesions correspond to fibroblasts proliferation area, surrounding with sclerotic or normal bone (5-9). The margin are, then, typically well-defined with a scalloped or serpentine configuration. When they are noted in children or young adults, these radiographic appearances are diagnostic. With aging, they are seen to migrate into diaphysis and fibro-osseous in-growth, becoming radiopaque and finally leading to normal bone. Ritshl’s classification is categorized into Stage A to D (2, 3, 6): Stage A, Eccentric lesion in the cortex which is small, oval to slightly polycyclic in shape without a sclerotic border. Stage B: Lesions with variable distance from the epiphysis with polycyclic shape and thin but clearly sclerotic borders; no periosteal reaction. Stage C: Lesions with properties similar to stage B but with also exhibit increasing sclerosis, which typically start from the diaphyseal side. Stage D 1–3: Complete homogeneous sclerosis of the lesion (D1), disappearing lesion (D2) and disappearance of the lesion (D3). Despite nonossifying fibroma is regarded as a “don’t touch” lesion, biopsy is occasionally conducted in case of FDG-PET markedly accumulating nonossifying fibroma mimicking metastatic bone tumor or in case of nonossifying fibroma with Stage B resembling other tumors such as giant cell tumors, aneurismal bone cyst or fibrous dysplasia (6-9). Nonossifying fibroma is basically benign. In most cases, treatment is not necessary and they typically go away on their own. In our case, bilateral cortical and subcortical bone defects with less than 2cm were found, indicating Stage A and B. Diffuse osteolytic lesions of the bone marrow at diaphysis in bilateral shinbones were also found. We are going to check these lesions periodically to assure not to be progressive.
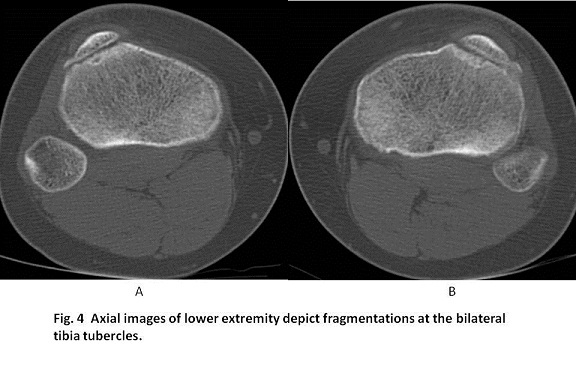
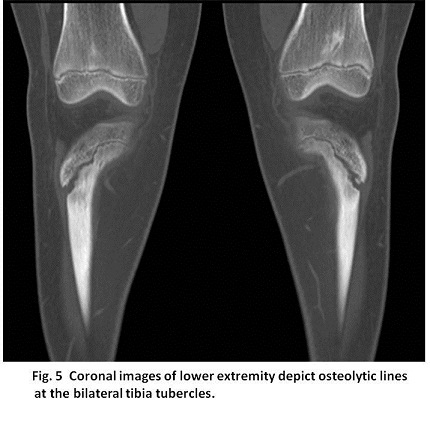
Osgood-Schlatter disease causes pain at the tibia tubercle- the bony bump where the patellar tendon attaches to the tibia (shinbone). It usually occurs in growing adolescents who conduct repetitive quadriceps contraction through the patella tendon, resulting from microtrauma of the patellar tendon and/or an avulsion of bone or cartilage in the tibial tuberosity (10 -14). In the growing process, the cartilage of the tibial tubercle extends inferiorly with its ossification. Occasionally, one or several ossification develops separately in the cartilage of the tibia tubercle (10-14). These finally connect together with main tibial epiphyseal ossification. Therefore, the presence of multiple osteous nodules anterior to the tibial mataphysis is a normal variant. Soft-tissue edematous change at the tibial tubercle enables to make Osgood-Schlatter disease and radiographic confirmation for the diagnosis is not necessary (10-14). In our case, CT was conducted for identification of the suspicious bone tumor but not for the confirmation of Osgood-Schlatter disease. CT showed the ossification of the cartilage of the tubercle is elongated and fragmented in both tibias, extending inferiorly to the proximal tibia epiphysis, expecting the fusion sooner or later (Fig. 3, 4).
【Summary】
We present a thirteen-year-old boy with painful proximal tibia, corresponded to tibia tubercle. Based on the clinical symtoms, Osgood-Schlatter disease was diagnosed. CT showed multiple osteolytic lesions within 2cm in size accompanied without and with thin sclerotic margins, indicating fibrous cortical defect (nonossifying fibroma), Stage A and B. Nonossifying fibroma is known to occur with the incidence of 30 % in adolescents and is found by chance. Nonossifying fibroma is known to migrate from metaphysis to diaphysis and categorized into four stages; Stage A, osteolytic lesion; Stage B, osteolytic lesion with thin sclerotic margin; Stage C, mixed with osteolytic lesion and osteosclerotic lesion; Stage D, complete homogeneous sclerosis. The images of elongate and fragmented ossification of tibia tubercle are considered to be a normal variant.
【References】
1.Mirra JM. Fibrohistiocytic tumors of intramedullary origin. In: Mirra JM, eds. Bone tumors: clinical, radiologic and pathologic correlation.Philadelphia, Pa: Lea & Febiger, 1989; 691-800.
2.Ritschl P, et al. Fibrous metaphyseal defects--determination of their origin and natural history using a radiomorphological study. Skeletal Radiol. 1988;17(1):8–15.View ArticlePubMedGoogle Scholar
3.Ritschl P, et al. Fibrous metaphyseal defects. Orthopade. 1995;24(1):44–9.
4.Hudson TM, Stiles RG, Monson DK. Fibrous lesions of bone. Radiol Clin North Am. 1993;31:279–97.[PubMed]
5.Kumar R, et al. Fibrous lesions of bone. RadioGraphics. 1990;10:237–56.[PubMed]
6.Ritschl P, et al. Fibrous metaphyseal defects. Magnetic resonance imaging appearances. Skeletal Radiol. 1989;18:253–29. [PubMed]
7.Brenner RJ, et al. Scintigraphic features of nonosteogenic fibroma. Radiology.1979;131:727–30. [PubMed]
8.Greyson ND, et al. The variable bone scan appearances of nonosteogenic fibroma. Clin Nucl Med.1981;6:242–45. [PubMed]
9.Moser RP, et al. Multiple skeletal fibroxanthomas: radiologic-pathologic correlation of 72 cases. Skeletal Radiol. 1987;16:353–59. [PubMed]
10.Dupuis CS, et al. Injuries and conditions of the extensor mechanism of the pediatric knee. Radiographics. 2009 May-Jun. 29(3):877-86. [Medline].
11.Rosenberg ZS, et al. Osgood-Schlatter lesion: fracture or tendinitis? Scintigraphic, CT, and MR imaging features. Radiology. 1992 Dec. 185(3):853-8. [Medline]. [Full Text].
12.Pretell-Mazzini J, et al. Outcomes and Complications of Tibial Tubercle Fractures in Pediatric Patients: A Systematic Review of the Literature. J Pediatr Orthop. 2015 Apr 10. [Medline].
13.Nakase J, et al. Relationship between the skeletal maturation of the distal attachment of the patellar tendon and physical features in preadolescent male football players. Knee Surg Sports Traumatol Arthrosc. 2012 Dec 22. [Medline].
14.Kaya DO, et al. Long-term functional and sonographic outcomes in Osgood-Schlatter disease. Knee Surg Sports Traumatol Arthrosc. 2013 May. 21(5):1131-9. [Medline].
2017.3.8
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.