

Clinical diagnosis
Case 48
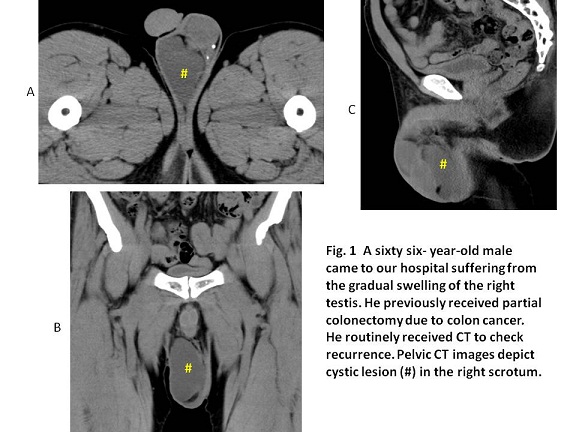
Case 1 (Fig. 1): He received no treatment because of no symptoms and being tolerable in size.
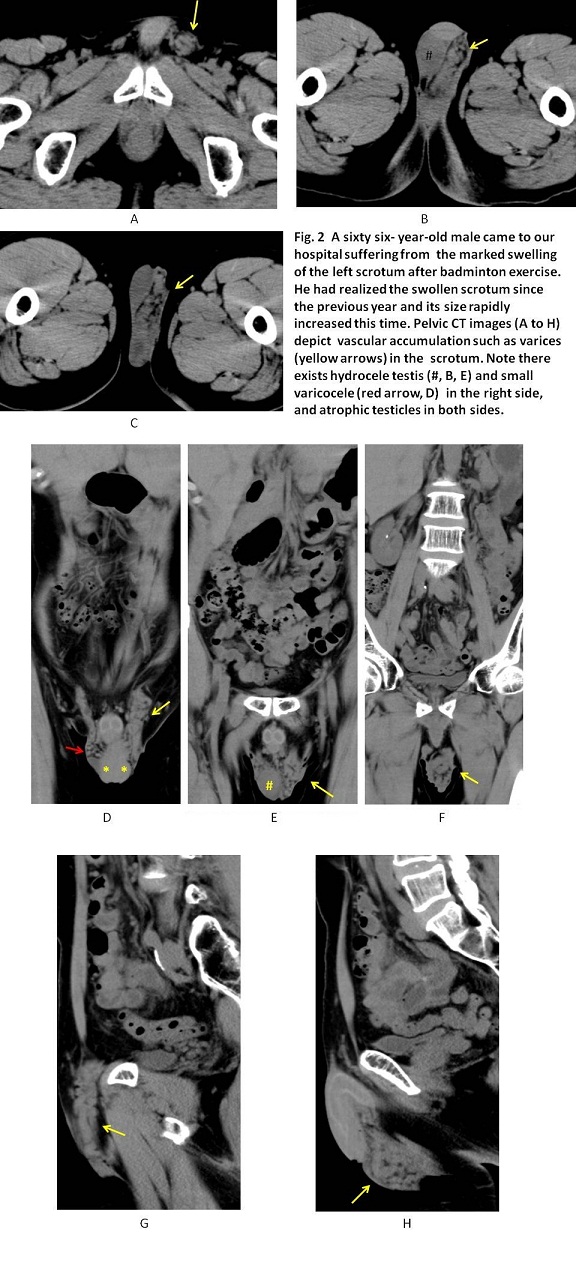
Case 2 (Fig. 2): He received surgical ligation of the testicular vein, inducing shrinkage of varicocele.
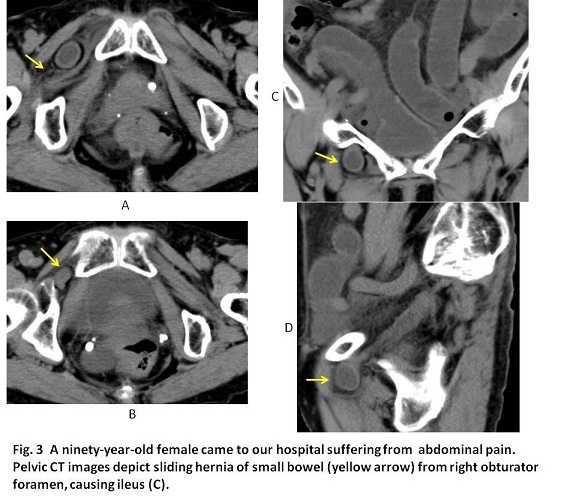
Case 3 (Fig. 3): She received surgical resection of the herniated content and closure of the hernia gates.
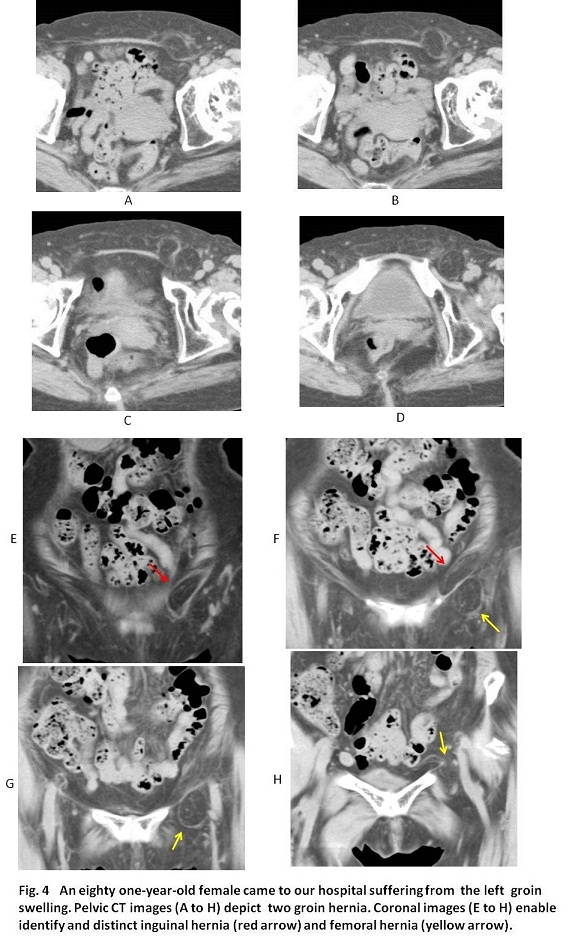
Case 4 (Fig. 4): She received surgical repair the following day. Twenty days later, she discharged without complication.
【Discussion】
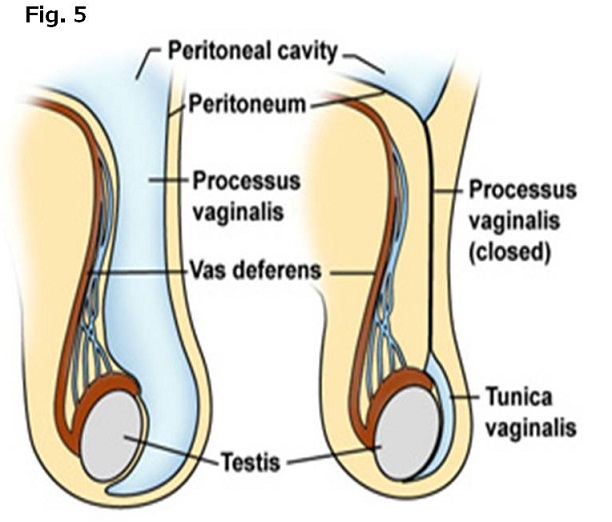
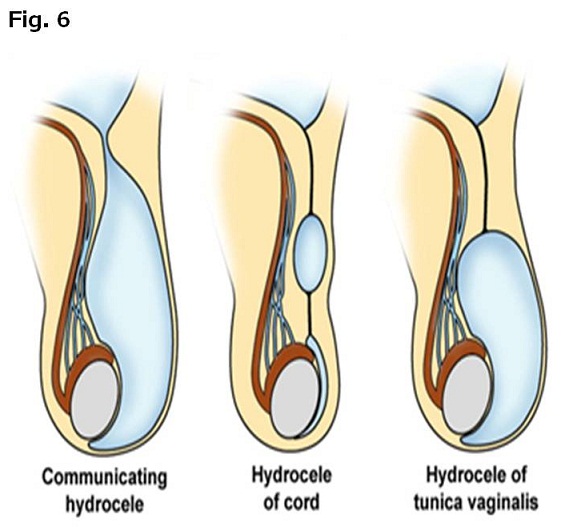
During fetus, the testis descends from peritoneum to scrotum via inguinal canal. At the early stage, the testis pressures the peritoneum forming like a diverticulum and then, the diverticulum extends into the scrotum, forming like a sheath, termed the processus vaginalis. In a normal pattern, the processus vaginalis following the testis descending is obliterated within two weeks before or after birth (1, 2). The peritoneal tissue enclosing testis and epididymis is named tunica vaginalis (精巣鞘膜) (Fig. 5) which is composed of two layers. A hydrocele testis is an accumulation of fluid which occurs in the opening space of the tunica vaginalis. Although the primary cause of a hydrocele testis is not clarified, it is considered to be owing to the incapable absorption of fluids. Three kinds of the hydrocele testis are known: Hydrocele of the tunica vaginalis, Hydrocele of the cord and Communicating hydrocele (Fig. 6). Indirect inguinal hernia and varicocele indicate increased risk in the scrotum (1, 2). In our cases, hydrocele testis was detected in Cases 1 and 2 whose types are Hydrocele of the tunica vaginalis and hydrocele of the cord, respectively. In Case 2, varicocele was detected in both sides of scrotum and a hydrocele testis is detected in the right side.
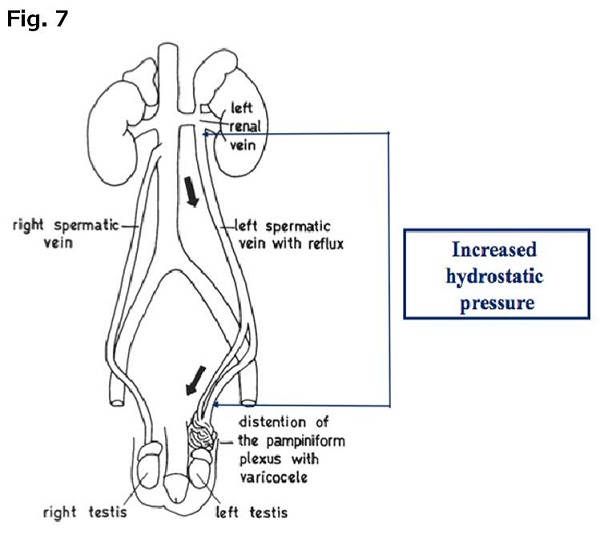
Varicocele (精索静脈瘤) mostly occurs on the left side because of the anatomical reason: the left testicular vein outflows to the left renal vein at a right angle indicating the blockade of the blood flow, while the right testicular vein directly outflows to the inferior vena cava, indicating negative pressure works to suck easily (Fig. 7)(3-6). The anatomical blockade is considered to cause the disorder of the testicular vein valves. When it occurs on the right side, it is usually seen on the both sides. Varicocele is listed one of the main infertility of the males, 30 % in couples who cannot have children (5). The temperature of the scrotum is several degrees lower than body temperature. It is believed that congestion of varicocele raises the temperature of the scrotum, inducing the negative effect on sperm production (6). In fact, it induces the atrophy of the testicles (5, 6). The grading of varicocele is categorized; Grade I, varicocele is palpable during or after Valsalva maneuver; Grade II, varicocele is palpable without the need for Valsalva maneuver: Grade III, varicocele is visible to the eye. In our case, varicoceles were found on the both sides on CT, Grade III on the left varicocele, Grade I on the right side. Atrophic change of the both testicles was found (Fig. 2D).
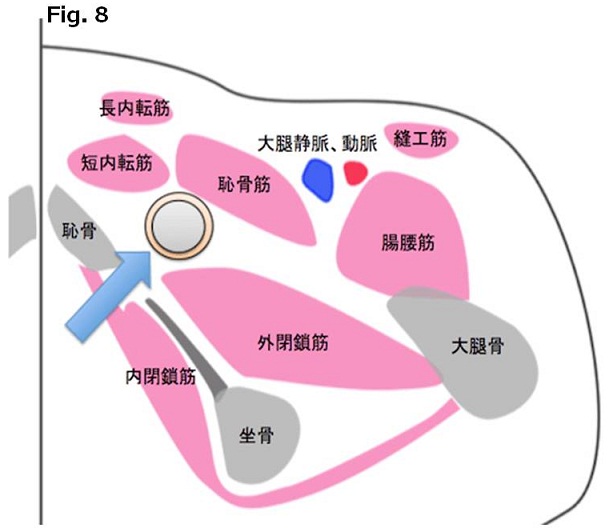
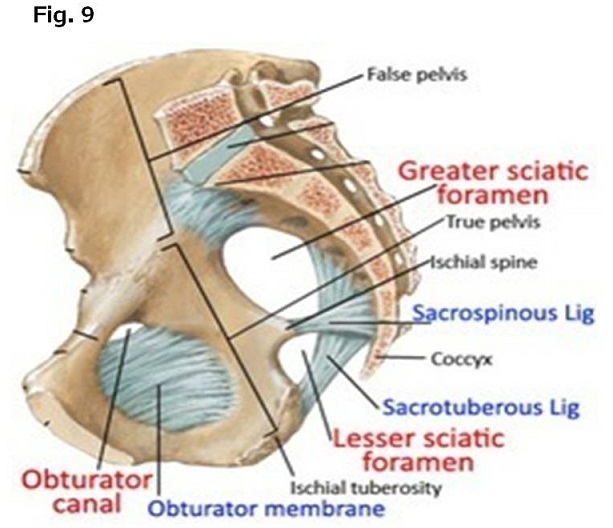
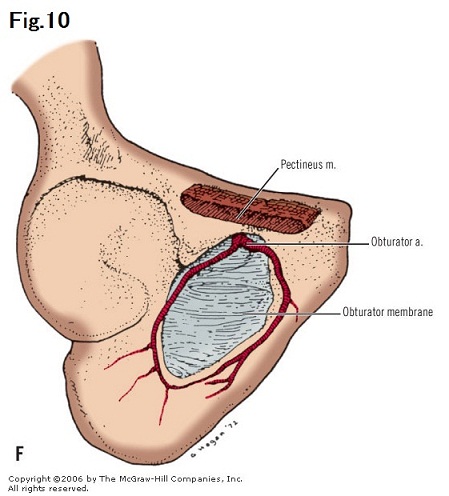
The obturator foramen is basically closed with three layers, internal obturator muscle, obturator membrane and external obturator muscle (Fig. 8). These layers are pierced by the canal composed of neurovascular bundle: obturator artery, vein and nerve (Figs. 9, 10). The peritoneum extends into the canal along with neurovascular bundle. Because obturator hernia occurs in a elderly woman, it is considered that relaxation of the pelvic peritoneum results from the previous pregnancy. Because of the existence of the sigmoid colon on the left side, the obturator hernia is predominant to occur on the right side. The well-known Howship-Romberg sign of medial thigh numbness which was caused by nerve compression of the bowel at the obturator canal, is present in approximately half of cases (7, 8). In our case, the obturator hernia was found in an elderly woman on the right side with ileus and not accompanied with Howship-Romberg sign.
Of the groin hernias, femoral hernia occurs in 6 %, while inguinal hernia, in 94% (9, 10). Femoral hernia is common in woman accounting for 70 % (9, 10). It is possible to have femoral hernia and inguinal hernia at the same time. Although the difference between inguinal hernia and femoral hernia is difficult on axial images, coronal (frontal) images are critical and easy to differentiate them. Namely, the inguinal hernia gate opens at the ventral side of the inguinal ligament, while femoral hernia gate opens at the dorsal side of the inguinal ligament. Continuous coronal CT helps us to find the hernia gate opening above or below the inguinal ligament. Approximately half of all femoral hernias are found as emergent cases (9, 10). In our case of an elderly woman, continuous coronal CT images showed the femoral hernia and indirect inguinal hernia, simultaneously. The both herniated contents are fatty tissue, probably mesentery or omentum. As the symptom was tolerable, the waiting surgery was possible to supply in case4.
【Summary】
We present 4 cases of testis hydrocele, varicocele, obturator hernia and both inguinal and femoral hernias. We should keep in mind that testis hydrocele occurs in the opening space of tunica vaginalis owing to the incapable absorption of fluids, that varicocele mostly occurs on the left side because of the anatomical reason that the testicular vein out flows to the left renal vein at a right angle indicating the possible blockade of the blood flow and raises the temperature, leading to the main cause of male infertility, that obturator hernia comes out of the neurovascular bundle and is likely to occur on the right side in an elderly woman, and that the differentiation between femoral hernia and inguinal hernia is to check whether those hernia gates open above or below the inguinal ligament on continuous coronal CT images.
【References】
1.Esposito C. Incidence and management of hydrocele following varicocele surgery in children. JUrol. 171 (3):1271–3. doi:10.1097/01.ju.0000112928.91319.fe. PMID 14767329.
2.Shan CJ, et al. A Comparative study of sclerotherapy with phenol and surgical treatment for hydrocele. J Urol. 2003; 169: 1056–9. doi:10.1097/01.ju.0000052680.03705.40. PMID 12576845.
3.F Yao, David. Male infertility: lifestyle factors and holistic, complementary, and alternative therapies. Department of Urology, UCLA. 2015;18: 410–8. doi:10.4103/1008-682X.175779. PMC 4854092 . PMID 26952957. Retrieved 23 March 2016.
4.Eisenberg, ML, et al. Varicocele-induced infertility: Newer insights into its pathophysiology. Indian Journal of Urology : IJU : Journal of the Urological Society of India. 27 (1): 58–64. doi:10.4103/0970-1591.78428. ISSN 0970-1591. PMC 3114589 . PMID 21716891.
5.Kupis Ł, et al. Varicocele as a source of male infertility - current treatment techniques. Cent European J Urol. 2015; 68: 365–70. doi:10.5173/ceju.2015.642. PMC 4643713 . PMID 26568883.
6.Song, GS. Could sperm quality be affected by a building environment? A literature review. Building and Environment. 2010; 45 : 936–943. doi:10.1016/j.buildenv.2009.09.016.
7.Aguirre DA, et-al. Abdominal wall hernias: imaging features, complications, and diagnostic pitfalls at multi-detector row CT. Radiographics. 25 (6): 1501-20. doi:10.1148/rg.256055018 - Pubmed citation
8.Cubillo E. Obturator hernia diagnosed by computed tomography. AJR Am J Roentgenol. 1983;140 (4): 735-6. AJR Am J Roentgenol (citation) - Pubmed citation.
9.Kitami M, Takase K, Tsuboi M et-al. Differentiation of femoral and inguinal hernias on the basis of anteroposterior relationship to the inguinal ligament on multidimensional computed tomography. J Comput Assist Tomogr. 2009;33 (5): 678-81. doi:10.1097/RCT.0b013e3181977a0a - Pubmed citation
10.Cherian PT, Parnell AP. The diagnosis and classification of inguinal and femoral hernia on multisection spiral CT. Clin Radiol. 2008;63: 184-92. doi:10.1016/j.crad.2007.07.018 - Pubmed citation
2017.3.29
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.