

Clinical diagnosis
Case 51
After admission, she was administered Veniron I (human immunoglobulin) of doses: 400mg/kg/day. However, the disorder of motor nerve system was getting worsened. Further, swallowing disturbance gradually occurred. Our reference doctor determined to send her to an expert hospital treating Guillain-Barre syndrome for more appropriate managements
【Discussion】
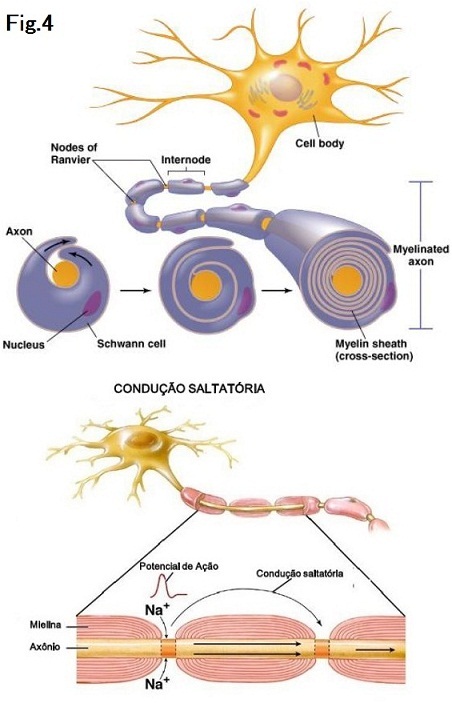
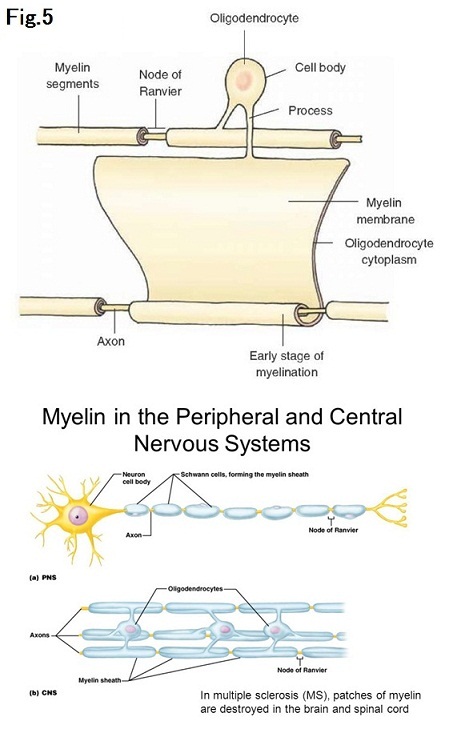
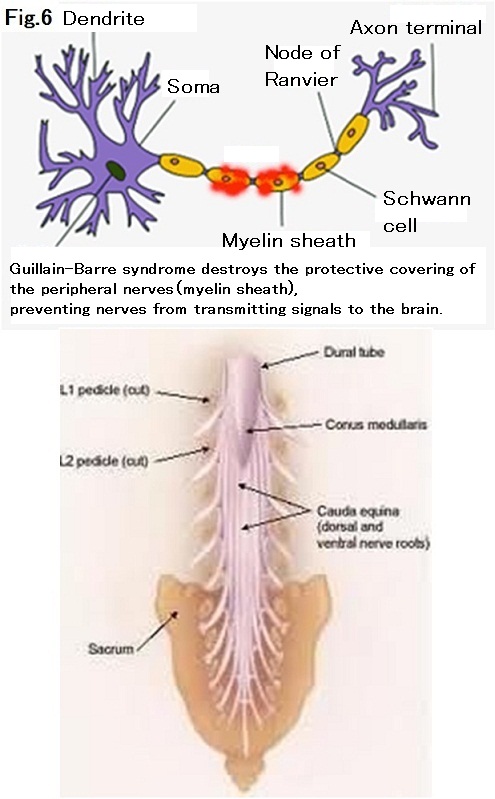
Guillain-Barre syndrome is an autoimmune-disorder that attacks a part of peripheral nerve. A peripheral nerve composes of parts of myelin (sheath), axon and swan cells (Fig.4). Peripheral nerves include cranial nerves, spinal nerves and autonomic nerves. Central nervous system composed of brain and spinal cord is not directly involved by Guillain-Barre syndrome as opposed to multiple sclerosis (1, 2)(Fig.5). The cause of this syndrome is not totally clarified. However, the recent researchers found that although the preceding infection was not always experienced, self-antibodies are originally,created responding to the preceding infection such as campylobacter, cytomegarovirus, EB virus and mycoplasm attack and damage to self-myelin and/or self-axon (1-4) (Fig.6). In case of campylobacter, the antigen of the bacteria and gangliosid of the peripheral nerve has a common molecular structure, implying that the self-antibody responded to campylobacter becomes to attack the peripheral nerve itself (3, 4). In our case, she ate the superficially-burned chicken and experienced severe diarrhea for several days. When diarrhea getting ceased, weakness of lower extremities began, suggesting the trigger of campylobacter infection.
The onset incidence of Guillain-Barre syndrome per year is not reported in Japan but 1 or 2 in 100,000 Americans, according to the National Institute of Neurological Disorders and Stroke (1, 2). The onset incidence of Guillain-Barre syndrome after campylobacter infection is 1 in 1000 (3, 4). The immune disorder is triggered by an infection or less vaccination. In 1976, influenza (H1N1) vaccination was conducted for 43 million people in the USA to prevent pandemic infection and thereafter, approximately 400 people fell into Guillain-Barre syndrome including 25 were dead (5). Our city has approximately 50,000 population, we might encounter one case with Guillain-Barre syndrome /one year or two years.
Guillain-Barre syndrome is mainly categorized into three types; acute inflammatory demyelinating polyneuropathy (AIDP) which involves selectively myelin composed of phospholipid layer surrounding the axon and functioning to insulate electrically; acute motor axonal neuropathy (AMAN) which involves selectively axon composed of the extension of the nerve cells functioning to carry nerve electric signals: acute motor and sensory axonal neuropathy (AMSAN) which involve both motor and sensory axons. In Japan, the incidences of AIDP and AMAN are approximately the same 40%, while in Europe and USA, the incidence of AMSAN is 90 % (1, 2).
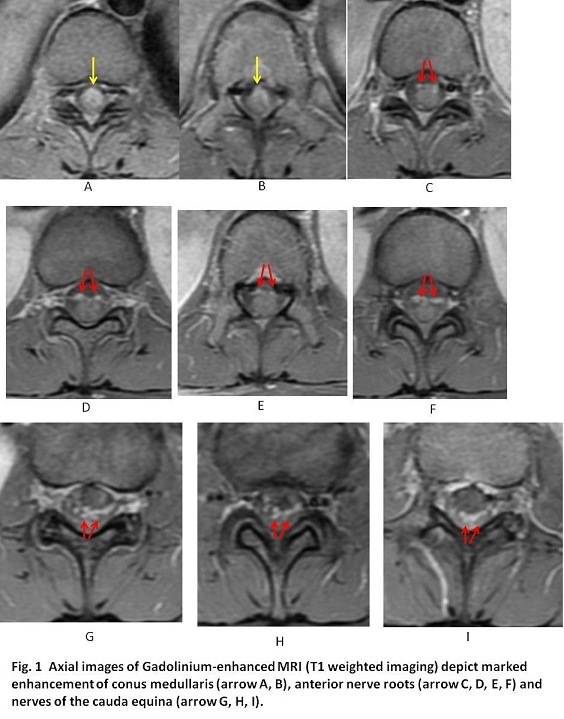
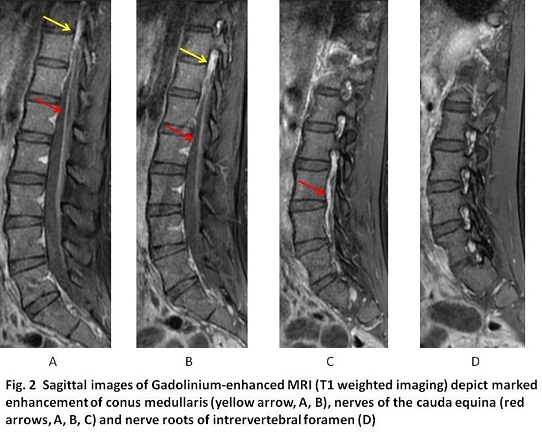
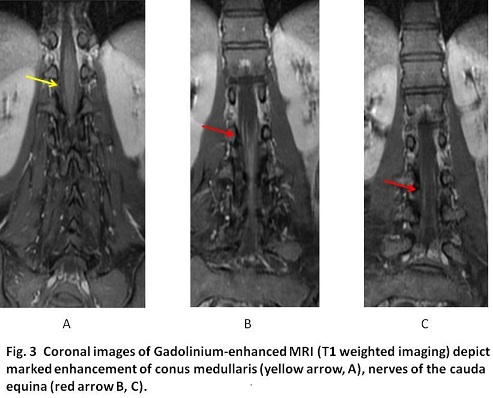
In order to investigate the radiological presence of Guillain-Barre syndrome, it is essential to use Gadolinium (Gd)-enhanced MRI because non-enhanced sequences of MRI are normal. Typical findings are prominent Gd-enhancement of the conus meddularis, anterior nerve roots and nerves of the cauda equine (6 – 9). In the cranial nerves, facial nerve (VIII) is most commonly affected (6). Although the Gd-enhancement of the spinal nerve roots can be found in inflammatory process such as polyneuropathy, neurosarcoidosis or arachnoditis, the enhancement of only the anterior spinal nerve roots is strongly suggestive of Guillain-Barré syndrome (9). In our patient, Gd-enhanced T1weighte image showed marked enhancement of the conus meddularis, anterior roots, nerves of eqina cauda and nerve radicles, implying typical Guillain-Barre syndrome.
【Summary】
We present a twenty five-year-old female with Guillain-Barre syndrome. She experienced selective paralysis of lower extremities after severe diarrhea for several days after ingestion of half-burned chicken, sugestive campylobacter infection. Gd-enhanced T1weighted imaging showed marked enhancement of conus meddularis, anterior nerve roots, nerves of cauda equine and nerve radicles in the intra-vertebral foramen, implying Guillain-Barre syndrome. We should keep in mind that Guillain-Barre syndrome selectively involves mainly motor nerves of peripheral nerves but not central nervous system as opposed to multiple sclerosis, and Gd-enhanced MRI is essential because non-enhanced MRI sequences are normal.
【References】
1.Dimachkie MM, et al. Guillain-Barré Syndrome and Variants. Neurol Clin. 2013 May; 31(2): 491–510. Published online 2013 Feb 19. doi:10.1016/j.ncl.2013.01.005
2.Logullo F, et al. Asymmetric Guillain-Barré syndrome. NEUROLOGICAL SCIENCES. 27:355-359 (2006) abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/17122
3.Church Potter R, Kaneene JB. “A descriptive study of Guillain-Barré syndrome in high and low Campylobacter jejuni incidence regions of Michigan: 1992-1999.” NEUROEPIDEMIOLOGY. 22:245-248 (2003) abstract available online at http://www.ncbi.nlm.nih.gov/pubmed/12792145
4.Ogawara K, Kuwabara S, Mori M, et al. Axonal Guillain-Barré syndrome: relation to anti-ganglioside antibodies and Campylobacter jejuni infection in Japan. Ann Neurol. 2000 Oct;48(4):624–631. [PubMed]
5.Lehmann HC, et al. Guillain-Barré syndrome after exposure to influenza virus.、、Lancet Infect Dis. 2010:10(9):643-51. Review.PMID 20797646
6.Fulbright RK, et-al. Cranial nerve enhancement in the Guillain-Barré syndrome. AJNR Am J Neuroradiol. 1995;16 (4): 923-5. AJNR Am J Neuroradiol (abstract) - Pubmed citation
7.Alkan O, Yildirim T, Tokmak N et-al. Spinal MRI findings of guillain-barré syndrome. J Radiol Case Rep. 2009;3 (3): 25-8. doi:10.3941/jrcr.v3i3.153 - Free text at pubmed - Pubmed citation
8.Li HF, Ji XJ. The Diagnostic, Prognostic, and differential value of enhanced MR imaging in Guillain-Barre syndrome. AJNR Am J Neuroradiol. 2011;32 (7): E140. doi:10.3174/ajnr.A2620 - Pubmed citation
9.Byun WM, et al.. Guillain-Barré syndrome: MR imaging findings of the spine in eight patients. Radiology. 1998 ;208:137-141
2017.4.19
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.