

Clinical diagnosis
Case 52

Ophthalmoscopy revealed bilateral eye ball infection, finding fungus balls. She was given four kinds of antibiotics after admission for several days. Because the blood culture revealed Streptococcus β infection, ceftriaxon and gentamycin were continued to use. Transthoracic echo did not find the emboli at the mitral valve or the left atrial appendage. Transesophageal echo was not conducted. Her consciousness was recovered, fever decreased, and hemiparesis was getting improved, although skin red eruption remained for a while. A week later, brain MRI was conducted again and showed no new infarction.
【Discussion】
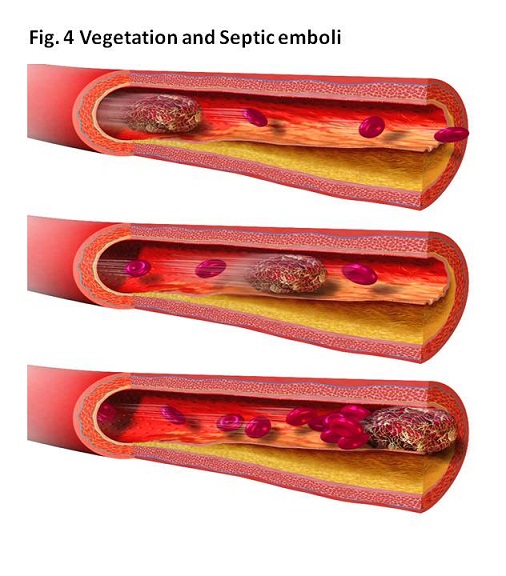
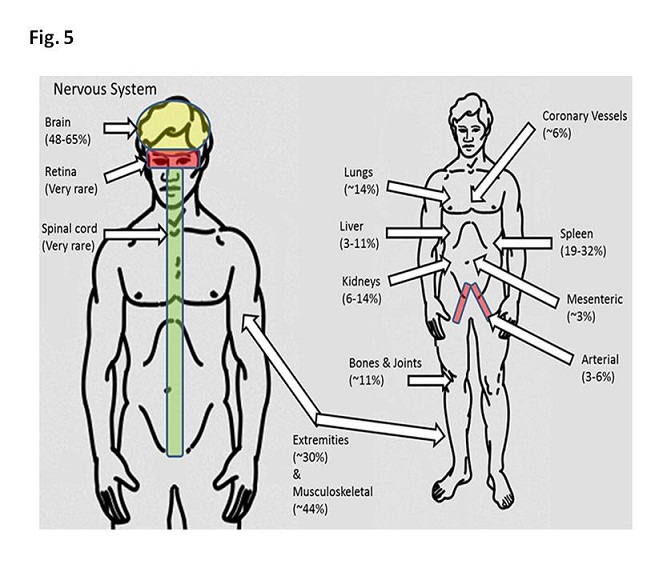
Approximately a half of all cases with infectious endocarditis had no known history of valvular disease (1, 2). Cardiac valves do not have a dedicated arterial blood supply system. Then, when an organism attaches to the valve, defensive immune system to resist bacteria does not respond effectively. As a result, bacteria proliferate and form a vegetation (bacillus accumulation + clot) (Fig. 4), travelling to the various parts of the body (Fig. 5). Meanwhile, in case of endothelial damage, platelet-fibrin clot, first occurs on the damaged endothelium and thereafter, bacillus from bactremia adheres to the clot, inducing to form a vegetation.
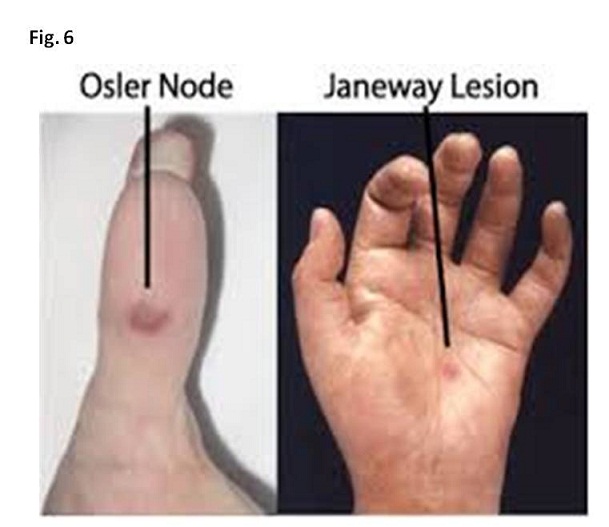
There exist two routes of septic emboli from left-sided endocarditis and right-sided endocarditis. Namely, when bacillus vegetation is formed on tricuspid valve or right ventricular endothelium, pulmonary septic emboli happen, while when bacillus vegetation is formed on mitral valve, aortic valve, left arterial appendage or left ventricular endothelium, systemic septic emboli happen in various body parts such as brain, retina, spleen, kidney, intestine and extremities (3 – 5). As specific findings observed in septic emboli from left-sided endocarditise, painless hemorrhagic cutaneous lesions on the palm and soles are named Janeway lesions (Fig. 6), painful subcutaneous lesions in the distal fingers are named Osler’s nodules (Fig. 6) and fungus ball in the retina are named Roth’s spots (Fig. 7) (3). In our case, changes by septic emboli appeared in brain, eye ball and upper and lower extremities including Janeway lesions.
Although any bacteria possibly cause endocarditis, Staphylococcus and Streptococcus are the main organisms. Staphylococcus infection is known to cause fulminant illness such as valvular fistula previously categorized acute bacterial endocarditis, while Streptococcus infection causes mild to moderate illness previously categorized subacute bacterial endocarditis (2 – 4). In our case, blood culture revealed Streptococcus infection. The prompt and appropriate use of antibiotics is imperative to control infectious endocarditis. She was given four kinds of antibiotics from admission and two antibiotics were omitted after the report of blood culture.
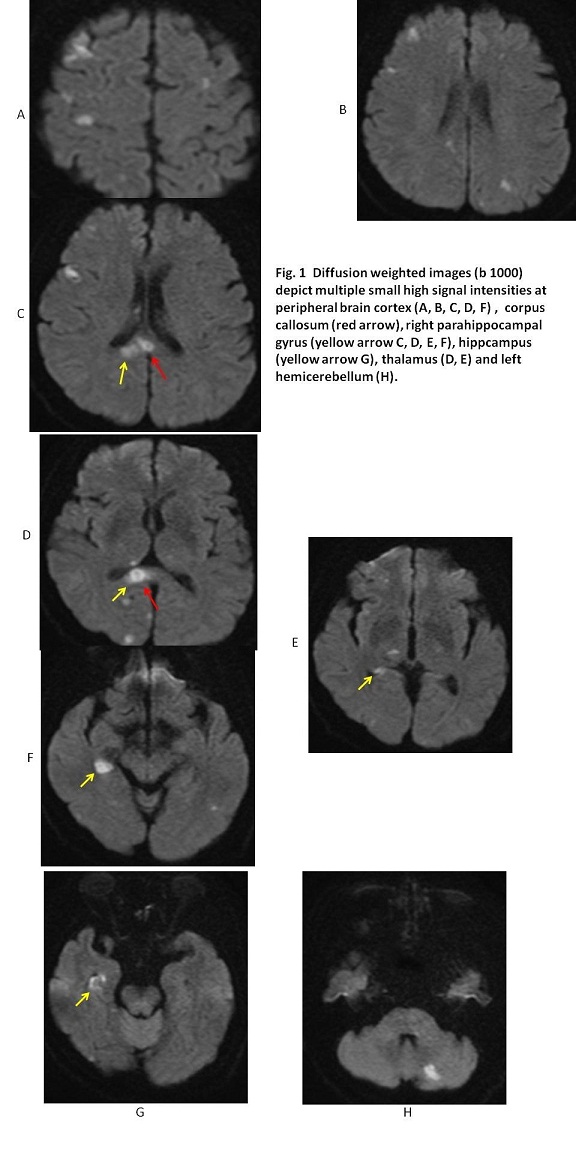
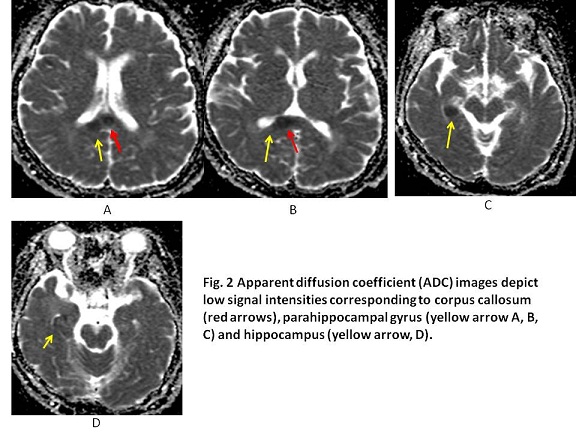
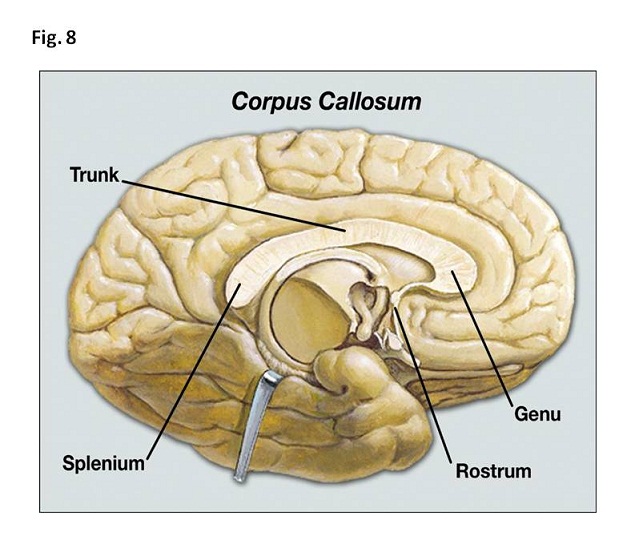
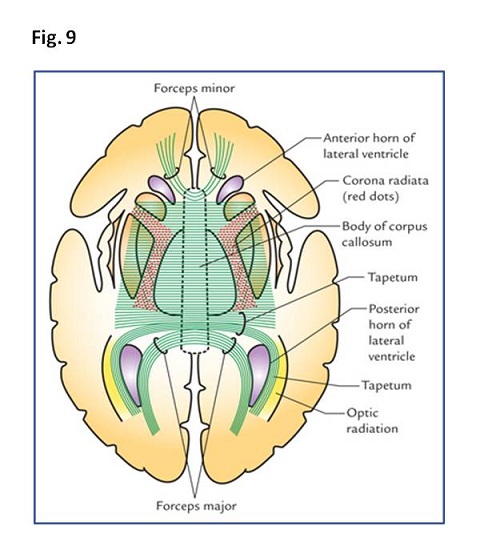
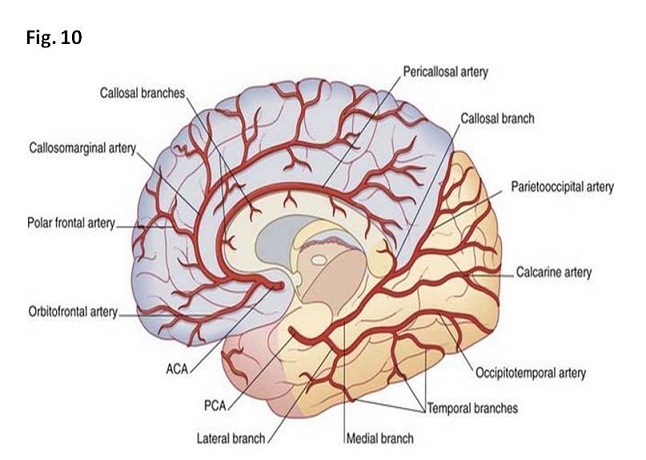
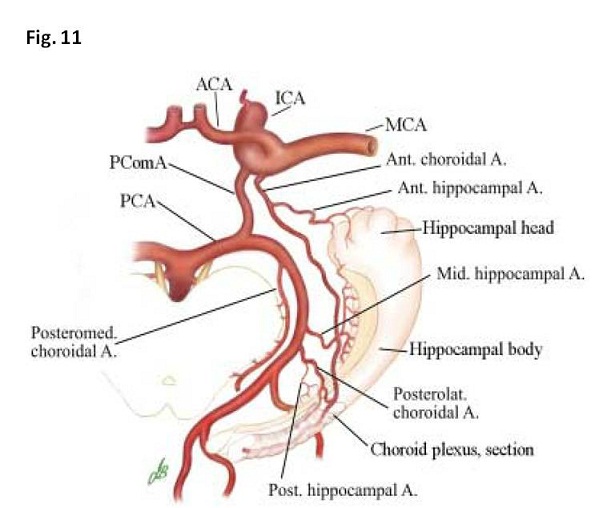
In our case, brain MRI showed multiple high signal intensities in peripheral cortex of cerebrum and cerebellum, splenium of corpus callosum, a small portion of parahippocampal gyrus and anterior and posterior portions of hippocampus. Corpus callosum composes of rostrum, genu, trunk and splenium (Fig. 8) whose fibers connect orbital cortex, frontal cortex, parietal cortex and posterior cortex, respectively (Fig. 9). Corupus callosum situates in the center of the human brain, forms the largest white matter bundle in the brain. It functions to communicate between left and right cerebral hemispheres, and integrate the information. The blood supply of splenium of corpus callosum is a tiny dorsal pericallosal branch from posterior cerebral artery (6) (Fig. 10). Hippocampus and parahippocampal gyrus are components of a limbic system whose ischemic damages rarely occur. Anterior part of hippocampas is supplied from anterior hippocampal branch from anterior choroidal artery arising from internal carotid artery. Meanwhile, parahippocampal gyrus and posterior part of hippocampas is supplied from posterior hippocampal branch arising from posterior cerebral artery (Fig. 11) (7). The lumens of both anterior and posterior hippocampal branches are very small, indicating the sizes of bacillus vegetation were tiny in our case.
【Summary】
We present a seventy seven-year-old female with septic emboli probably from a left-sided endocarditis. She had no episode of mitral valve disease. She experienced fever, disorder of consciousness, transient hemiparesis, transient left abducent nerve palsy, eye ball infection and multiple skin red eruptions including Janeway lesion. Blood culture revealed streptococcus infection. Brain MRI showed multiple small high signal intensity in peripheral cortex of cerebrum and cerebellum including small portion of right splenium of corupus callosum and small portions of anterior and posterior parts of right hippocampas and parahippocampal gyrus. We should keep in mind that hipoocampal head and body is supplied from anterior choroidal artery and hippocampal tail and parahippocampal gyrus are supplied from posterior hippocampal branch and dorsal hippocampal branch arising from posterior cerebral artery.
【References】
1.Heiro M, et al. Infective endocarditis in a Finnish teaching hospital: a study on 326 episodes treated during 1980–2004. Heart. 2006; 92: 1457–62. doi:10.1136/hrt.2005.084715. PMC 1861063
2.Morris AM. How best to deal with endocarditis. Curr Infect Dis Rep. 2006 8 (1): 14–22. doi:10.1007/s11908-006-0030-8. PMID 16448596.
3.Kasper DL, Brunwald E, Fauci AS, Hauser S, Longo DL, Jameson JL (2005). Harrison's Principles of Internal Medicine. McGraw-Hill. pp. 731–40. ISBN 0-07-139140-1. OCLC 54501403.
4.Stawicki SP, et al. Septic embolism in the intensive care unit. Int J Crit Illn Inj Sci. 2013 Jan-Mar; 3: 58–63. doi: 10.4103/2229-5151.109423
5.Avery RK, et al. Listeria monocytogenes tricuspid valve endocarditis with septic pulmonary emboli in a liver transplant recipient. Transpl Infect Dis. 1999;1:284–7. [PubMed]
6.Fitsiori A, et al. The corpus callosum: white matter or terra incognita. Br J Radiol. 2011 Jan; 84(997): 5–18. doi: 10.1259/bjr/21946513
7.Lüdemann W, et al. Arterial supply of the temporo-medial region of the brain: significance for preoperative vascular occlusion testing. Surg Radiol Anat. 2001;23(1):39-43.
2017.4.26
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.