

The appropriate choice
Case 54
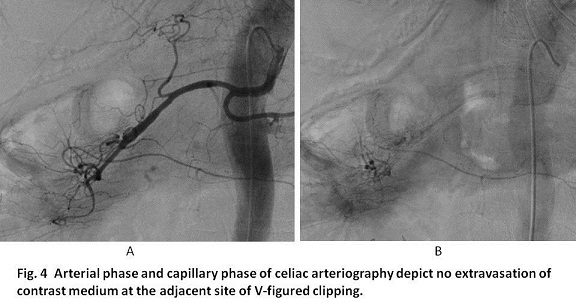
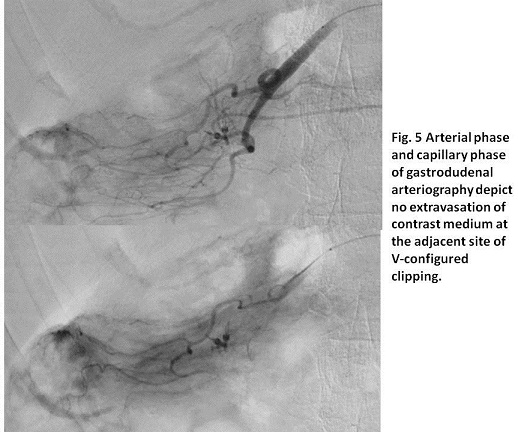
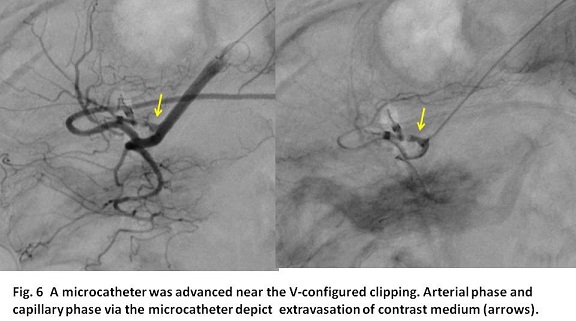
【Embolization】As a strategy, a 4F shepherd fuck catheter system without a sheath was used because a 3F catheter system is not appropriate for microcoil embolization although the smaller puncture site is more preferable in the coagulopathic condition. Celiac arteriography and gastroduodenal arteriography did not show any extravasation of contrast medium (Figs 4, 5). Then, a microcatheter was advanced to the distal gastroduodenal artery near V-configured clipping placed in endoscopy. Angiography via the microcatheter showed ulcer-type pseudoaneurysm directly from gastroduodenal artery (Fig. 6).
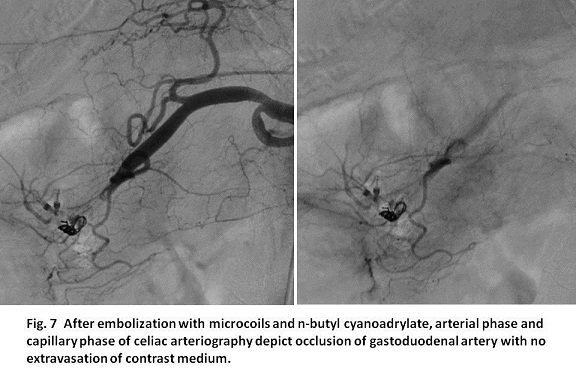
Then, the distal site of the pseudoaneurysm was occluded using two microcoils via the microcatheter. Thereafter, NBCA embolization was attempted. Namely, 5 % glucose was filled in the microcatheter using a 3-way stop-cock and the mixed solution of 1:2 of NBCA versus lipiodol was infused so as to fill the pseudoaneurysm plus connecting gastroduodenal artery. Celiac arteriography after embolization showed the occlusion of the gastroduodenal artery preserving patency of the posterior and anterior superior pancreaticoduodenal arteries (Fig. 7).
Thereafter, no recurrent bleeding happened. She received medicine for duodenal ulcer for three weeks in our hospital and was transported to the local hospital for rehabilitation of Parkinson disease.
【Discussion】
As embolic materials currently used in clinical situations, gelatin sponge particles (Serescue, Spongel or Gelfoam), microcoils and NBCA are listed. Gelatin sponge particles and NBCA are preferred for distal embolization, while coil embolization is preferred for proximal embolization of main branches from aorta. When gelatin sponge particles are infused in the vessels, secondary thrombosis adhesive to GSP in the normal or mild coagulopathic condition enhances occlusive durability. GSP injected into an artery for embolization is absorbed with secondary thrombus into the vessel wall within 2 weeks (1, 2). However, the scarce thrombosis in a severe coagulopathic condition, the secondary thrombosis does hardly occur, implying that recanalization of the occluded artery occur soon (3, 4). In our case, embolization with gelatin sponge particles was not attempted because the hemorrhage was not from the peripheral site but the relatively proximal site, gastroduodenal artery, indicating the insufficient occlusion potency of the gelatin sponge particles.
Microcoil is a permanent embolic material and especially feasible for ceasing arterial bleeding directly from the main branch of aorta such as gastroduodenal artery or proper hepatic artery. The bleeding point can be isolated by placing microcoil to both of the proximal and distal sites leading to occlusion. Microcoil of 0.014 inch in diameter through a micro-catheter has prevailed instead of coil of 0.035 inch thanks to technological innovation. However, a lumen of a 3F catheter is still narrow for passing a microcoil of 0.014 inch microcatheter,Then, a 4F catheter system is necessary for microcol embolization. In our case, we inserted a 4F catheter without a sheath because acquiring the puncture size as small as possible.
NBCA is highly regarded as useful embolic material to occlude and eradicate arteriovenous malformation, fistula, and pseudoaneurysm (5 - 7). Although NBCA itself is monomer, NBCA is polymerized with anion such OH- or Cl- in plasma or saline which is termed polymerization, resulting in instant permanent occlusion, and can be identified under X-ray fluoroscopy when mixed with lipiodol. Then, after making a mixture of lipiodol and NBCA, 5% glucose using a 3-way stopcock has to inject to fill the microcatheter. A 3-way stopcock is essential to prevent backflow of blood into the catheter tip. Further, NBCA owns occlusion potency in a coagulopathic condition with platelet counts less than 50,000/mm3 and or PTINR>1.5. In our case, PTINR was 1.37 which was near the coagulopathic condition and embolization with NBCA was more preferable rather then embolization with gelatin sponge particles. Further, the arterial bleeding came directly from the gastroduodenal artery. First, a microcatheter was inserted to the distal site and microcoil embolization of the distal site was conducted. Although isolation to occlude the bleeding site was possible using the more microcoils, we intended to occlude pseudoaneurysm itself using NBCA.
【Summary】
We present an eighty two-year-old female with active duodenal bleeding. Successful endoscopy hemostasis was achieved twice but endoscopic physicians were afraid of re-hemorrhage because of potent hemorrhagic tendency. Celiac angiography and proximal gastroduodenal angiography showed no evidence of extravasation of contrast medium but distal gastroduodenal angiography via the microcatheter selectively advanced to near the site of V-shaped clipping placed for hemostasis in endoscopy, revealed pseudoaneurysm extended directly from gastroduodenal artery. Embolization with microcoil and NBCA was conducted, resulting in the permanent occlusion. We keep in mind that gelatin sponge particles and NBCA are preferred for distal embolization, while coil embolization is preferred for main branches from aorta such as proper hepatic artery or gastroduodenal artery. Further, in case of coagulopathic condition such as platelet counts less than 50,000/ mm3 and or PTINR > 1.5, embolization with NBCA is more preferable rather than embolization with gelatin sponge particles.
【References】
1.Nakatsuka H. Nonsurgical intraarterial gelatin sponge injection: experimental and clinical investigation of an anticancer procedure. Osaka City Medical Journal 1979; 28:191-223.
2.Sato M, Yamada R. Experimental and clinical studies on the hepatic artery embolization for treatment of hepatoma. Nippon Acta Radiologica 1983; 43:977-1005.
3.Yonemitsu T, Kawai N, Sato M, Tanihata H, Takasaka I, Nakai M, Minamiguchi H, Sahara S, Iwasaki Y, Shima Y, Shinozaki M, Naka T, Shinozaki M: Evaluation of transcatheter arterial embolization with gelatin sponge particles, microcoils, and n-butyl cyanoacrylate for acute arterial bleeding in a coagulopathic condition. J Vasc Interv Radiol 20(9): 1176-1187, 2009
4.Yonemitsu T, Kawai N, Sato M, Sonomura T, Takasaka I, Nakai M, Minamiguchi H, Sahara S, Iwasaki Y, Naka T, Shinozaki M: Comparison of hemostatic durability between N-butyl cyanoacrylate and gelatin sponge particles in transcatheter arterial embolization for acute arterial hemorrhage in a coagulopathic condition in a swine model. Cardiovasc Intervent Radiol 33(6): 1192-1197, 2010
5.Wikholm G. (1995) Occlusion of cerebral arteriovenous malformations with N-butyl cyano-acrylate is permanent. Am J Neuroradiol 16:479-482.
6.Sanchez MJ, Ananian CL, Berkmen T (2006) Embolization of an arch pseudoaneurysm with coils and N-butyl-cyanoacrylate. J Vasc Interv Radiol 17:1677-1679.
7.Yamakado K, Nakatsuka A, Tanaka N, et al (2000)Transcatheter arterial embolization of ruptured pseudoaneurysms with coils and N-butyl cyanoacrylate. J Vasc Interv Radiol 11:66-72.
2017.5.17
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.