

Clinical diagnosis
Case 60
【Diagnostic background】
Case 1(Figure 1): Alcohol abuse and long-term history of drinking alcohol. Alcoholic liver disorder: total bilirubin 2.5 mg/dL.
Case 2 (Figure 2): Alzheimer disease. Hasegawa test score 10 (< 20), mini-mental score examination, failed
Case 3 (Figure 3): Alcohol abuse and long-term history of drinking alcohol. Alcoholic liver disorder, Inarticulate speaking, IQ 32.8. Hasegawa test score 21(< 20), MMSE 24 (< 23), indicating to retain some cognition. possible Welnicke syndrome.
Case 4 (Figure 4): Alzheimer disease. VSRAD 3.8 (< 2.0).
【Discussion】
The longer alcohol use is known to cause negative effects on liver and central nervous system. The mechanism of the negative effects such as chronic liver disease and brain shrinkage is not fully understood yet. Homocysteine level is elevating in the patients with alcohol withdrawal symptoms. Homocysteine itself is a precursor of methionine which is much included in meats and dairy products and can convert to methionine with assistance of methyl donors of vitamin Bs 6, 9 and 12. If these vitamins are lacking or excessive amounts of alcohol or coffee, there is a risk of building up homosyteine. There are some reports elevating evidence that homocysteine induces neural cell damage via simulation to N-methyl-D-asparate (NMDA) receptors related to neural cell death and free radical (1, 2). Homocysteine might contribute to the pathogenesis of both brain shrinkage and alcohol withdrawal symtoms.
The imaging modality is useful to check the degree of brain shrinkage. Images of MRI show cerebral atrophy characterized by lateral and 3rd ventricular dilatation as well as cerebellar atrophy characterized by 4th ventricular dilatation in elderly patients with chronic alcoholism (3). Further, T2 weighted images of MRI show hyperintense lesions on deep white matter and/or periventrivular area with higher incidence in chronic alcoholism patients than adults of the same age and gender who are not alcoholic (3). Shrinkage of frontal lobe which is the site of higher intellectual functions is found in the excessive amount of alcohol consumed (4). Some studies documented an approximate positive correlation between shrinkage of mammilary body and memory loss (4, 5). Kubota M, et al. reported that alcohol consumption of more than 350g ethanol/ a week induce the consequent frontal lobe atrophy, while the moderate consumption of alcohol of average of 182g ethanol/a week did not affect frontal volume (6). It is documented that a few months of alcohol abstinence bring out gradual recovery of brain volume, cerebral blood flow and neuropsychological impairment (7, 8, 9).
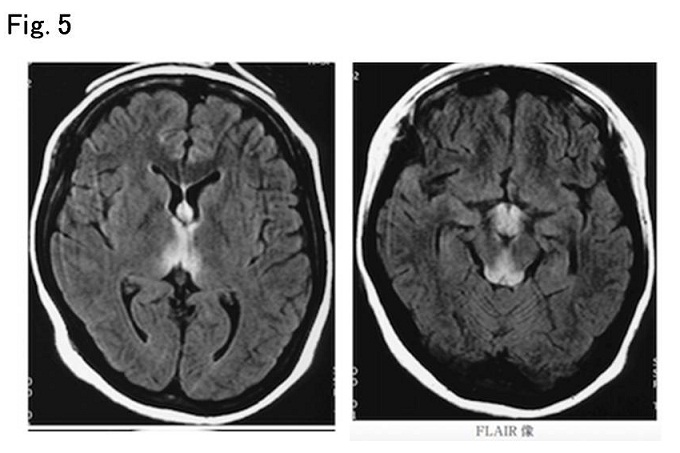
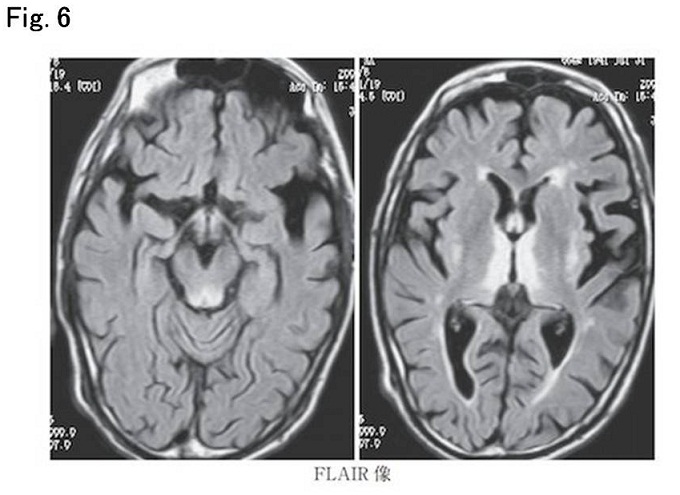
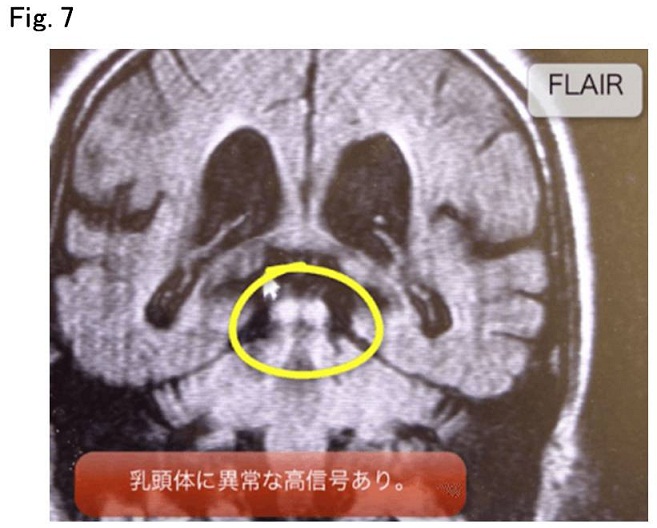
In MRI of Case 1 showed marked shrinkage of frontal lobe (Fig. 1) but not accompanied with the atrophy of amygdale body and entorhinal cortex which is relatively specific for Alzheimer disease (Figs 2 and 4) Wernicke-Korsakoff syndrome is caused by chronic alcoholism associated with thiamine (vitamin B1) deficiency. Wernicke-Korsakoff syndrome combines Wernicke’s encephalopathy: nystagmus, ataxia and confusion with Korsakoff syndrome: antegrade and retrograde amnesia (10). It involves damage to specific areas in the brain. Namely, it is known that in acute Wernicke’s encephalopathy, T2-weighted image and Gd-enhanced T1-weighted image show the hyper signal intensity at mammilary bodies, periventricular regions of third ventricle and periaqueductal regions (Figs 5 - 7). These changes are no longer visible in the chronic phase of Wernicke-Korsakoff syndrome.
In our Case 3, he suffered from chronic Wernicke-Korsakoff syndrome. MRI showed no hyper intense signal intensity on specific area but moderate shrinkage of non-specific atrophy of whole lobe with sparing amygdale and entorhinal cortex (Fig. 3). It is known that atrophy of medial aspect of temporal lobe is specific MRI findings for Alzheimer disease. In our Cases 2 and 4 (Figs 2 and 4) with Alzheimer disease, MRI showed marked atrophy of bilateral amygdale body and entorhinal cortex, corresponded to the medial sides of temporal lobe.
【Summary】
We present axial images on MRI in four patients; two patients with chronic alcoholism: two patients with Alzheimer disease. The difference of brain atrophy between them on MRI images was whether sparing of amygdale and entorhinal cortex or not. In short, the atrophy of amygdalate and entorhinal cortex is found in Alzheimer disease, but not in chronic alcoholism. However, it is possible that chronic alcoholism is associated with Alzheimer disease in elderly patients. In such a case, the atrophy of amygdalate and entorhinal cortex can be associated with the alcoholic atrophy. In our Case 3, MRI did not show typical images of Wernicke-Korsakoff syndrome probably because of a chronic type, although the typical image of an acute Wernicke-Korsakoff syndrome is reported to be hyper signal intensity at mammilary bodies, periventricular regions of third ventricle and periaqueductal regions. We should keep in mind that Homocysteine might contribute to the pathogenesis of alcoholic brain shrinkage, and that alcohol much consumed contribute the pathogenesis of whole cerebral brain atrophy and alcohol excessively much consumed contribute marked atrophy of frontal lobes.
【References】
1.Bleich S, et al. Homocysteine and alcoholism. J Neural Transm Suppl. 2000; 60:187-196.
2.Bleich S, et al. . Hyperhomocysteinemia as a new risk factor for brain shrinkage in patients with alcoholism". Neurosci. Lett. 2003; 335:179–82. doi:10.1016/S0304-3940(02)01194-1. PMID 12531462.
3.Hayakawa, K, et al. MR Imaging of Chronic Alcoholism. Acta Radiologica, 1992; 33: 201-206
4.Pfefferbaum A, Sullivan EV, Mathalon DH, Kim, KO. Frontal lobe volume loss observed with magnetic resonance imaging in older chronic alcoholics. Alcohol Clin Exp Res 1997;21(3):521-529.
5.Sullivan EV, et al. Cerebellar volume decline in normal aging, alcoholism, and Korsakoff's syndrome: relation to ataxia. Neuropsychology 2000;14:341-352.
6.Kubota M, et al. Alcohol consumption and frontal lobe shrinkage: study of 1432 non-alcoholic subjects. J Neurol Neurosurg Psychiatry 2001;71:104–106
7.Sullivan EV, Deshmukh A, Desmond JE, et al. Cerebellar volume decline in normal aging, alcoholism, and Korsakoff's syndrome: relation to ataxia. Neuropsychology 2000;14:341-352.
8.Fortman BJ, Kuszyk BS. Incidentally diagnosed Marchiafava-Bignami disease. AJR 1999;173(6):1713-1714.
9.Arbelaez A, Pajon A, Castillo M. Acute Marchiafava-Bignami disease: MR findings in two patients. AJNR 2003;24(10):1955-1957.
10.Thomson, Allan D, et al. The natural history and pathophysiology of Wernicke's Encephalopathy and Korsakoff's Psychosis. Alcohol and Alcoholism. 2006; 41: 151–158
2017.6.28
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.