

Imaging diagnosis
Case 66
【Progress】
He was given continuous antibiotics and diuretics. His symptoms fluctuated between clear consciousness with smiling and least response for three weeks. His temperature and blood pressure was getting lowered. Unfortunately, he passed away for senile decay 21 days after brain CT.
【Discussion】
The clinical symptoms of posterior reversible encephalopathy syndrome (PRES) are headaches, altered consciousness, visual disturbance and seizures (1). PRES can occur in all ages from 2 years to 90 years in the literature (1 – 5). The typical imaging finding is a vasogenic edema predominant in the subcortical parietal-occipital white matter. Our patient was 99 years old, probably the oldest case of the reported cases. His main symptom was altered consciousness. Brain CT showed hypoattenuation of bilateral posterior lobe.
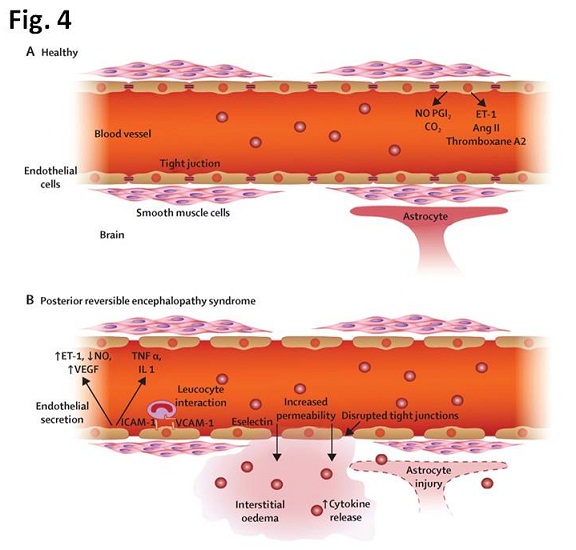
There are two theories of pathophisiology for causing posterior reversible encephalopathy syndrome (PRES): vasogenic (vascular) edema due to hypertension (Fig. 4) and endothelial disorder. PRESS is often found associated with acute high systolic pressure, such as chronic hypertension, renal disorder and eclampsia. Severe hypertension may exceed the limit of autoregulation, leading to hyperperfusion and breakthrough vasogenic edema. The reason why PRES is mainly involved in the bilateral posterior lobe is generally accepted to result from the relatively less sympathetic innervation of the vertebrobasilar circulation. In other words, the sympathetic innervative potency is maximal in the internal carotid artery territories thanks to carotid sinus (sensor of hypertension). Sympathetic mediated vasoconstriction may be more effective in the carotid artery circulation from overperfusion in case of acute hypertension than in the vertebral artery circulation. Because of this anterior to posterior gradient of sympathetic innervation, hyperperfusion state results in edema in the vertebral artery circulation territories.
However, less than 30% of patients have normal or only mildly raised blood pressure (2-6). Mechanism of endothelial dysfunction rather than vasogenic edema is documented. PRES is associated with inflammatory process such as sepsis, eclampsia, transplantation and autoimmune disease and exposure of immunosuprressive drugs or chemotherapy agents (1-6). The inflammatory process or systemic toxicity causes endothelial dysfunction. However, the theory of endothelial dysfunction does not explain why some cases of PRES seem to occur in the vertebral artery territories.
Our patient was not in the state of hypertension: his blood pressure was relatively low, less than 130 mmHg during the clinical course. He had pneumonia with pleural effusion which might have caused endothelial dysfunction.
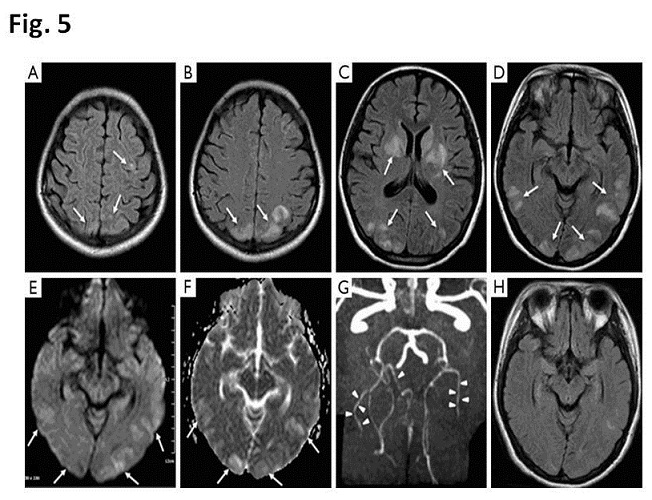
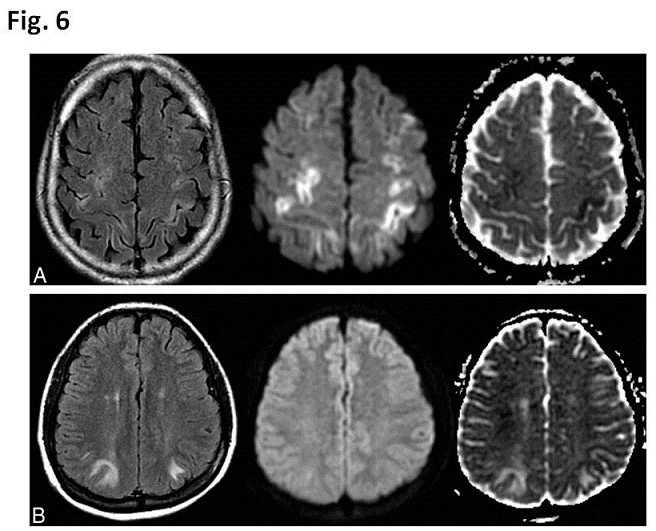
Typical neuro-image findings are symmetric white matter edema in the posterior cerebral hemisphere (98%), particularly water-shed region of the parietal-occipital region (1, 3) (Figs 5, 6.). Cerebellum and brain stem (30-53%) are occasionally involved associated with PRES (10-14). Abnormality in milder cases, was seen in the gray matter, implying the brain edema begin in the cortex. Neuro-imaging abnormality can be detected in brain CT. The standard modality to visualize PRES is MRI. The most commonly observed abnormality is the confluent high signal intensity of posterior area on Fluid-attenuated inversion recovery (FLAIR) or T2WI (12). It is also typical that the area consistent with high mobile water in areas of vasogeic edema in PRES increased (high) ADC values may appear hyperintense (Fig. 5), hypointense, or isointense (Fig. 6) on diffusion-weighted imaging (DWI), depending on the amount of the T2 “shine-through” effect.
High signal intensity on DWI and pseudonormalized ADC values seem to be correlated with cerebral infarction and may represent the earliest sign of irreversibility as severe vasogenic edema progresses to cytotoxic edema. Coexistence of hypointense and hyperintense lesions on ADC mapping of the affected areas is frequently observed (Fig. 6) but purely cytotoxic edema is also reported. Increased ADC values indicate vasogenic edema, most often reversible, while decreased ADC values indicate cytotoxic edema that inevitably induces cell death and progression to true infarction (12-15).
Further, gyrus-form enhancement is found on Gd-enhanced T1WI (1,3,13,14), implying disruption of blood brain barrier and tiny or large low signal intensity can occur on T2*, meaning that severe vasogenic edema might bring about cytotoxic damage and/or hemorrhage (15).
Unfortunately, we had no chance of supplying MRI in our case. However, brain CT showed bilateral confluent low density in posterior lobe not only white matter but also gray matter, implying brain edema.
PRES is also referred as Reversible posterior leukoencephalopathy syndrome (RPLS), Reversible posterior cerebral edema syndrome, Posterior leukoencephalopathy syndrome, Hyperperfusion encephalopathy and Brain capillary leak syndrome (1). None of these names is completely satisfactory; the syndrome is not always reversible, and it is often not confined to either the white matter or the posterior regions of the brain (1). In this presentation, we used posterior reversible encephalopathy syndrome (PRES) because of the familiar sound of PRES.
【Summary】
We present a ninety nine-year-old male suffering from altered consciousness. Brain CT showed confluent low density of bilateral posterior region implying brain edema, indicating typical CT image of PRES. Although brain MRI was not conducted, we should keep in mind that typical images of PRES are the confluent high signal intensity of posterior area on FLAIR or T2WI and slightly high signal intensity due to T2 shine through on DWI and high signal intensity on ADC maps, indicating vascular edema.
【References】
1.Hobson EV, et al. Posterior Reversible Encephalopathy Syndrome: A Truly Treatable Neurologic Illness. Perit Dial Int. 2012 Nov-Dec; 32(6): 590–594. doi: 10.3747/pdi.2012.00152
2.Hinchey J, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med 1996; 334:494–500 [PubMed]
3.Fugate JE, et al. Posterior reversible encephalopathy syndrome: associated clinical and radiologic findings. Mayo Clin Proc2010; 85:427–32 [PMC free article] [PubMed]
4.Gokce M, et al. Posterior reversible encephalopathy syndrome caused by hypertensive encephalopathy and acute uremia. Neurocrit Care 2006; 4:133–6 [PubMed]
5.Onder AM, et al. Posterior reversible encephalopathy syndrome in the pediatric renal population. Pediatr Nephrol 2007; 22:1921–9[PubMed]
6.Ergün T, et al. Recurrent posterior reversible encephalopathy syndrome in a hypertensive patient with end-stage renal disease. Diagn Interv Radiol 2008; 14:182–5[PubMed]
7.Naidu K, et al. Single photon emission and cerebral computerised tomographic scan and transcranial Doppler sonographic findings in eclampsia. Br J Obstet Gynaecol 1997; 104:1165.
8.Tajima Y, et al. Two similar cases of encephalopathy, possibly a reversible posterior leukoencephalopathy syndrome: serial findings of magnetic resonance imaging, SPECT and angiography. Intern Med 1999; 38:54.
9.Paulson OB, et al. Cerebral autoregulation. Cerebrovasc Brain Metab Rev 1990; 2:161.
10.Jones BV, et al. Hypertensive encephalopathy in children. AJNR Am J Neuroradiol 1997; 18:101.
11.Koch S, et al. Diffusion-weighted imaging shows cytotoxic and vasogenic edema in eclampsia. AJNR Am J Neuroradiol 2001; 22:1068.
12.Mukherjee P, et al. Reversible posterior leukoencephalopathy syndrome: evaluation with diffusion-tensor MR imaging. Radiology 2001; 219:756.
13.Lewis LK, et al. CT and angiographic correlation of severe neurological disease in toxemia of pregnancy. Neuroradiology 1988; 30:59.
14.Schwartz RB, et al. Hypertensive encephalopathy: findings on CT, MR imaging, and SPECT imaging in 14 cases. AJR Am J Roentgenol 1992; 159:379.
15.Ollivier M, et al. Neuroimaging features in Posterior Reversible Encephalopathy Syndrome: A Pictorial Review. Neurological Sceinces 10.1016/j.jns.2016.12.007
2017.8.9
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.