

Imaging diagnosis
Case 67
【Progress】
At the time of twenty days after admission, he suffered from continuous headache, requiring a regular medicine. He found himself a sense of difference like undefined and clouded. He could make a conversation and understand verbs. However, he was unable to comprehend a half of nouns. He could not understand the meaning of scissors. His higher functional dysfunction and headache made him tend to get angry and irritated. Although palsy of his left lower extremity was not recovered, he could get to walk 5 to 10 meters, thanks to rehabilitation. He was scheduled to continue rehabilitation and learn everything again while making a usual life after discharge.
【Discussion】
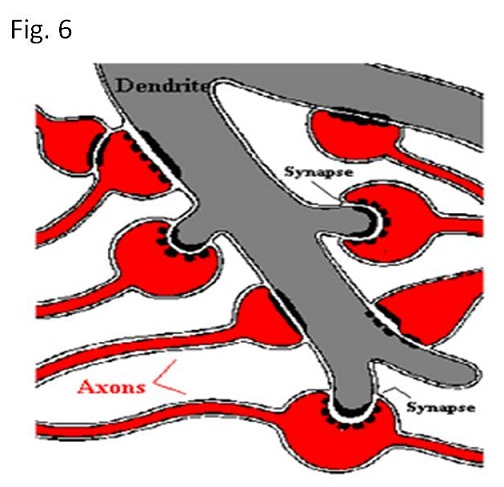
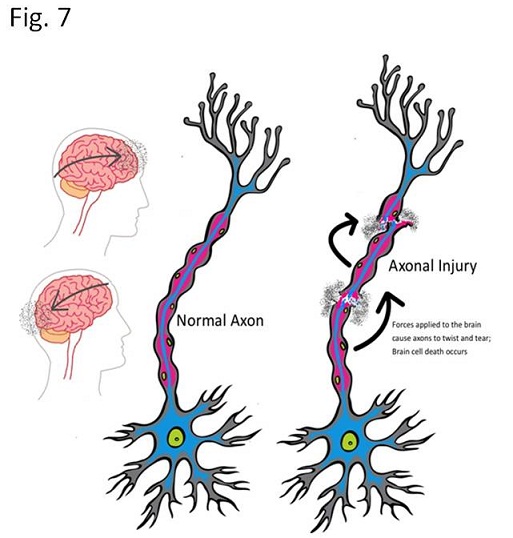
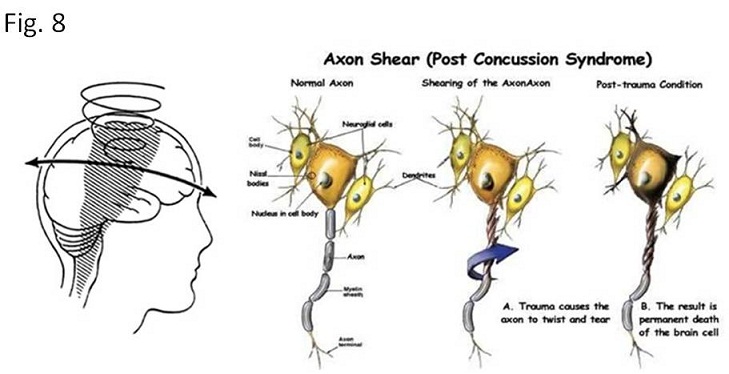
Neurons have axon and dendrites. Axon takes information away from the brain cell and dendrites bring information to the brain cell. Information from one neuron to another neuron flows across a synapse which contains a small gap with receptors and neurotransmitters (Fig. 6). Gray matter, brain cortex composes of brain cells, while white matter composes of neuron, mainly axon. There is a difference of density between white matter and gray matter. Namely, the density of white matter is a little heavier than that of gray matter. When whole brain is severely shaken such as traffic accident or child abuse (called post concussion syndrome), the interface between white matter and gray matter is susceptible to axon shear (Fig. 7)(1, 2). When severe concussion occurs, corpus callosum which is the largest white matter, linking the cerebral cortex of the right and left cerebral hemispheres, can be injured (Fig. 8)(1-5). Irrespective of skull fracture, subarachnoid hemorrhage, or subdural hemorrhage, this injury occurs in case of rapidly and repeatedly shaking and rotation due to sudden changes in velocity of the head (1, 2). Motor vehicle accident is a typical example. Also, in our case, motor traffic accident was a trigger of diffuse axon injury.
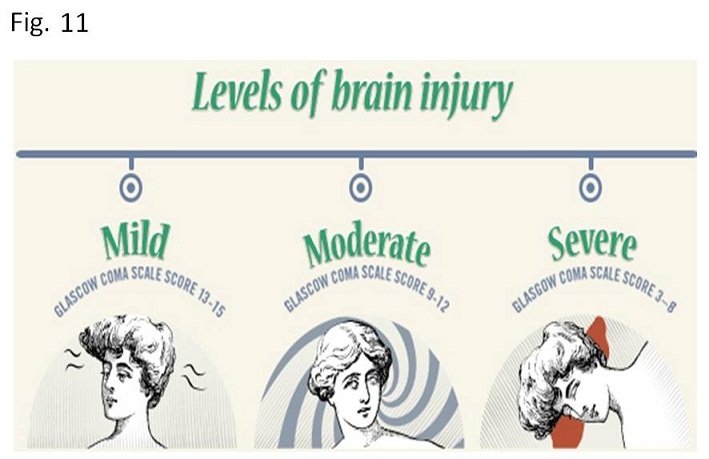
Frontal lobe, parietal lobe, occipital lobe and temporal lobe bear higher brain function. It is well known that frontal lobe is in charge of intellectual activities; parietal lobe in charge of movement, recognition and perception; occipital lobe in charge of visual processing: temporal lobe in charge of memory, auditory stimuli and speech. Then, the various degree of higher brain dysfunction can occur depending on the extent of axonal injury of the interface between the gray matter and white matter or large white matter. Glasgow coma scale for head injury which is most available in a clinical stage (mild, moderate and severe) of diffuse axonal injury, compose of eye movement, verbal response and motor response reflecting higher brain function (Figs. 9-11)(6). In our case, consciousness was recovered soon, indicating a mild stage of Glasgow coma scale and the disorder of parietal lobe (recognition, left lower extremity movement) was found.
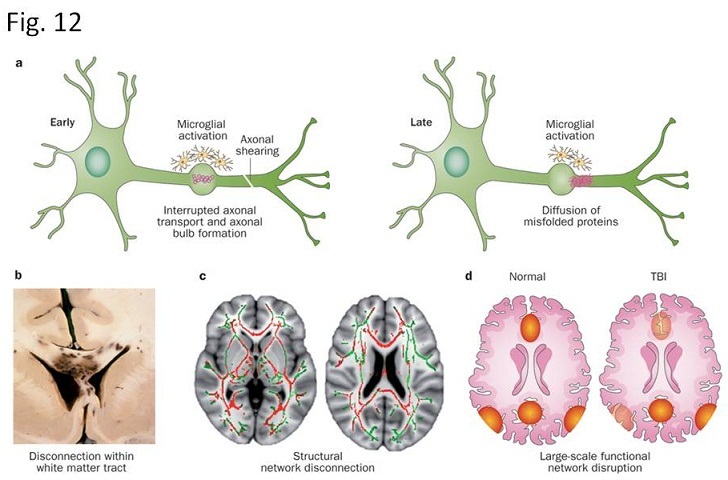
The recent literature said the axonal injury appears in two types; shear (tearing): stretch and a bulb formation followed by delayed secondary rupture due to biochemical reaction by microglia (Fig. 12)(7-9). Imaging modality of CT and MRI cannot always show the direct trauma of axonal injury, although higher brain functional was extremely disordered. Namely, CT can be normal or tiny hemorrhage of interface between cortex and white matter. MRI with diffusion weighted imaging and T2* is more sensitive to show the axonal damages such as micronecrosis and/or microbleeds rather than MRI with other MRI sequences (10-13). MRI with diffusion b1000 and T2* in our case showed micronecrosis and microbleeds, respectively mainly in the parietal lobe (Fig.3).
To date, there is no effective medicine for diffuse axon injury. As the late rupture of axon is dependent upon the chemical substance, the future target might explore the agent to repress the chemical substance. In experimental studies with total brain injury, progesterone brought about the significant improvement in neuron loss and behavior deficits, but yet to be clarified in clinical studies (14).


【Summary】
We present a thirty five-year-old male with diffuse axonal injury after traffic injury. He suffered from paralysis of left lower extremity and recognition disorder. CT showed tiny hemorrhage at the interface between cortex and white matter. MRI with diffusion weighted imaging b1000 showed tiny area of high signal intensity and T2* showed multiple micro-bleeds in the parietal lobe. At first, we were puzzled the reason why these tiny lesions caused the extensive higher brain dysfunction. We should keep in mind that repeated shaking and rotation cause axon injury especially at the interface between cortex and white matter, inducing early shear and bulb formation followed by late rupture by chemical substance. As a result, extremely higher brain injury appears in the late phase.
【References】
1. Tang-Schomer M.D. et al. Mechanical breaking of microtubules in axons during dynamic stretch injury underlies delayed elasticity, microtubule disassembly, and axon degeneration. FASEB J. 2010;24(5):1401–1410. [PMC free article] [PubMed]
2. Ahmed S.M. et al. Stretch-induced injury alters mitochondrial membrane potential and cellular ATP in cultured astrocytes and neurons. J Neurochem. 2000;74(5):1951–1960. [PubMedMeythaler J.M. et al. Current concepts: Diffuse axonal injury-associated traumatic brain injury. Arch Phys Med Rehabil. 2001;82(10):1461–1471. [PubMed]
3. Thomas M, Dufour L. Challenges of diffuse axonal injury diagnosis. Rehabil Nurs. 2009 Sep-Oct. 34(5):179-80. [Medline]
4. Povlishock J.T, Katz D.I. Update of neuropathology and neurological recovery after traumatic brain injury. J Head Trauma Rehabil. 2005;20(1):76–94. [PubMed]
5. Li X.-Y, Feng D.-F. Diffuse axonal injury: Novel insights into detection and treatment. J Clin Neurosci. 2009;16(5):614–619. [PubMed]
6. Teasdale G, Jennett B (1974). "Assessment of coma and impaired consciousness. A practicalscale." Lancet. 2 (7872):81–4. doi:10.1016/S0140-6736(74)91639-0. PMID 4136544
7. Johnson V.E, Stewart W, Smith D.H. Axonal pathology in traumatic brain injury. Exp Neurol. 2013;246(C):35–43. [PMC free article] [PubMed]
8. Loane D.J, et al. Role of microglia in neurotrauma. Neurotherapeutics. 2010;7(4):366–377. [PMC free article] [PubMed]
9. Oehmichen M, et al. Is traumatic axonal injury (AI) associated with an early microglial activation? Application of a double-labeling technique for simultaneous detection of microglia and AI. Acta Neuropathol. 1999;97(5):491–494. [PubMed]
10. Orrison W.W. et al. Traumatic brain injury: A review and high-field MRI findings in 100 unarmed combatants using a literature-based checklist approach. J Neurotrauma. 2009;26(5):689–701. [PubMed]
11. Provenzale J.M. Imaging of traumatic brain injury: A review of the recent medical literature. AJR Am J Roentgenol. 2010;194(1):16–19. [PubMed]
12. Liu J, Kou Z, Tian Y. Diffuse axonal injury after traumatic cerebral microbleeds: an evaluation of imaging techniques. Neural Regen Res. 2014 Jun 15. 9 (12):1222-30. [Medline].
13. Schrader H, et al. Magnetic resonance imaging after most common form of concussion. BMC Med Imaging. 2009 Jun 17. 9:11. [Medline]. [Full Text].
14. Shakeri M, et al. Effect of progesterone administration on prognosis of patients with diffuse axonal injury due to severe head trauma. Clin Neurol Neurosurg. 2013 Oct;115(10):2019-22. doi: 10.1016/j.clineuro.2013.06.013. Epub 2013 Jul 18.
2017.8.16
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.