

Clinical diagnosis
Case 7
【Progress】
After obtaining the informed consent, the patient was admitted and received a surgical laparotomy which revealed the strangulation ileus with volvulus of the small bowel without necrosis. The patient discharged without complication several days later.
【Discussion】
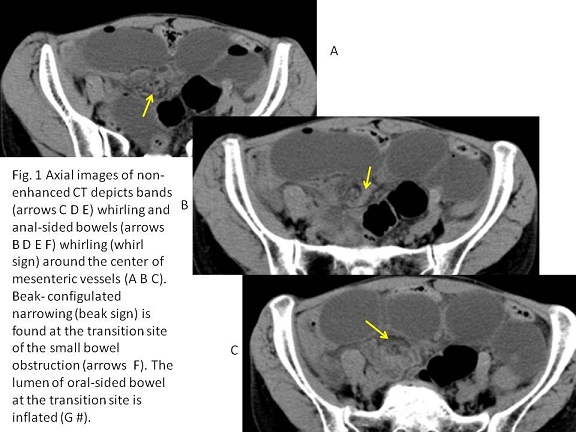
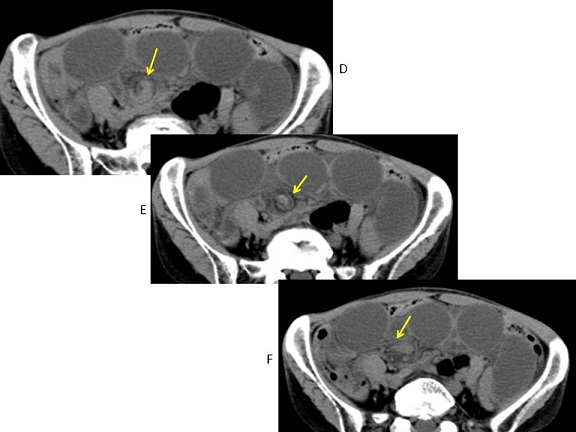
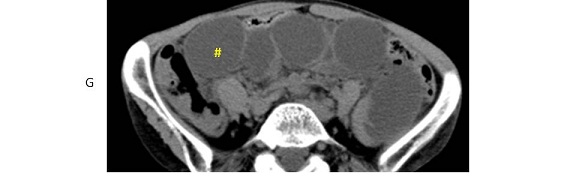
Strangulation ileus (volvulus) of small bowel is a life-threatening disease which requires an emergent surgical procedure (1-5). Speedy and accurate diagnosis of strangulation ileus is critical. When small bowel obstruction is encountered on CT, “whirl sign” and “beak sign” are helpful to differentiate simple ileus from strangulation ileus (1-5).
The whirl sign first documented by Fisher (4) was found at CT in a case of small bowel volvulus. The center of the whirl was the superior mesenteric artery (vessels) and the whirled appearance was created by the encircling loops of bowel (4). Patients with a ‘whirl sign’ on CT have a high probability of having small bowel obstruction, with a positive predictive value of 60 to 80%, and those without the sign probably do not have SBO, with a negative predictive value of 86 to 94 % (1-3). The Odd’s ratio for the ‘whirl sign’ predicting a small bowel obstruction necessitating surgery is reported to be 25.3(1). However, the whirl sign may not be as apparent if the axis of rotation is not perpendicular to the transverse scanning plane (4, 5). Then, not only the axial images but also the coronal and sagittal images should be created for image interpretation.
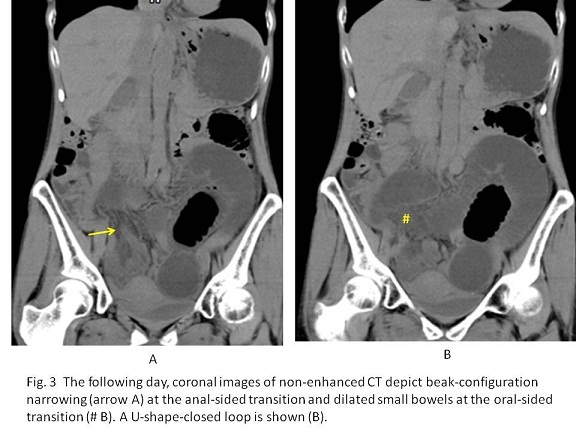
The beak sign is appeared as the tapering narrowing of oral-sided and anal-sided small bowels at the occlusive point and often associated with the “whirl sign”(1-5). Because the oral-sided small bowel is dilated filled with air and the anal-sided bowel is contracted, the beak sign tends to be found at the occlusive point of the anal-sided bowel.
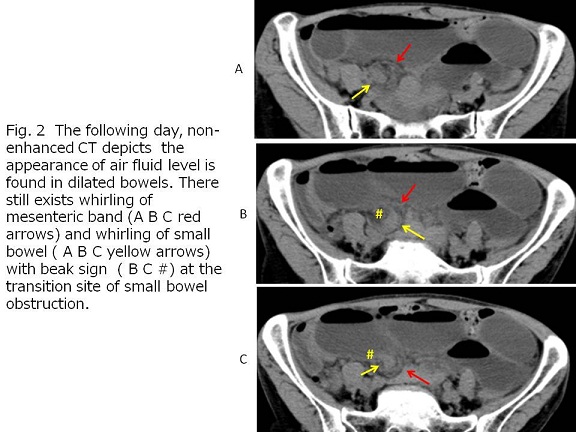
Strangulation ileus results in ischaemia or infarction. Clinical signs are not always reliably predictive for the need for surgical intervention in strangulation ileus, and delay in treatment is a major prognostic factor for survival and morbidity (1, 2, 5). The mortality rates for gangrenous ileus range significantly higher than those for non-gangrenous ileus (1). In our case, although the results of laboratory test were subtle, CT depicted whirl sign and beak sign, leading to the treatment of surgical laparotomy with no resection of the small bowel.
【Summary】
A sixty-year-old female with a chief complaint of epigastric pain received abdominal CT twice which depicted the gradual dilatation of small bowel, the whirl sign and the beak sign, making the diagnosis of early strangulation ileus although subtle abnormal laboratory data was found, and leading to the surgical laparotomy which revealed no necrosis of the small bowel.
【References】
1.Duda JB, Bhatt S, Dogra VS. Utility of CT whirl sign in guiding management of small-bowel obstruction. AJR Am J Roentgenol 2008;191:743-747.
2.Khurana B. The whirl sign. Radiology 2003:226:69-70.
3.De Korte N, Grutters CT, Snellen JP. Small bowel volvulus diagnosed by the CT ‘whirl sign’. J Gastrointest Surg 2008:12(8):1469-1470. Epub 2007 Oct 20.
4.Fisher JK. Computed tomographic diagnosis of volvulus in intestinal malrotation. Radiology 1981; 140:145-146.
5.Kuehnast M, et al. Pictorial interlude: Caught up in a ‘whirl. S Afr J Surg 2012;50:50-51.
2016.05.25
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.