

Answer
Case 73
【Progress】He was admitted as connective tissue disease-associated interstitial lung disease. He was given high-dose oral corticosteroid (1 mg/kg body weight of oral prednisone) and his dyspnea was getting improved. Tapering of corticosteroid therapy was conducted. He was discharged one month later with regular small dose of corticosteroids per day.
【Discussion】
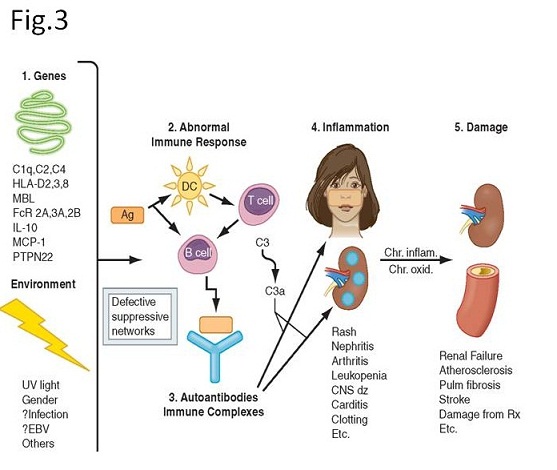
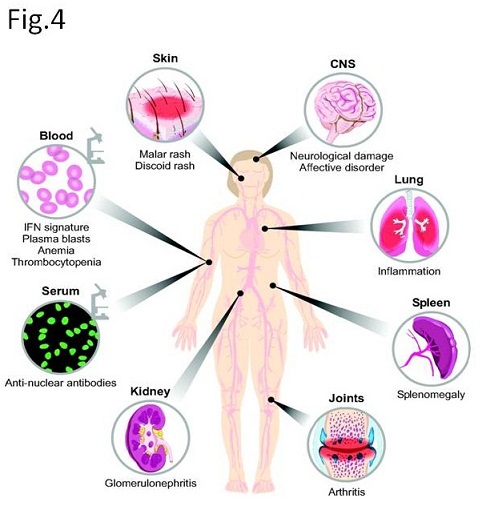
Anti-double stranded DNA IgG antibody (anti-ds DNA IgG antibody) is an antibody to self-DNA with double strand. Its highly positive value is specific for active systemic lupus erythematosus (SLE). The value of was 292 (< 10) IU/mL in our case. Although etiology of SLE is still not fully clarified, the occurrence of SLE is related with defects in the clearance of apoptotic cells. Apoptotic cells are engulfed by macrophages in the early stage of apoptotic cell death under healthy condition, leading to no occurrence of inflammation or immune response. This clearance mechanism is impaired in patients with SLE (1). Possible clearance defects are listed; complement deficiencies; defects in macrophage handling: inducing self-antigen in apoptotic cells exposed to T cell or B cell (Fig. 3). The disorder of clearance mechanism is found not only in the peripheral blood but also in the lymphnodes (1). Then, complex of self-antigen and self-antibody injure self-whole body, causes inflammation of skin rash, nephritis, arthritis and vasculitis and leads to damages to systemic organ including pulmonary fibrosis (Fig. 4).
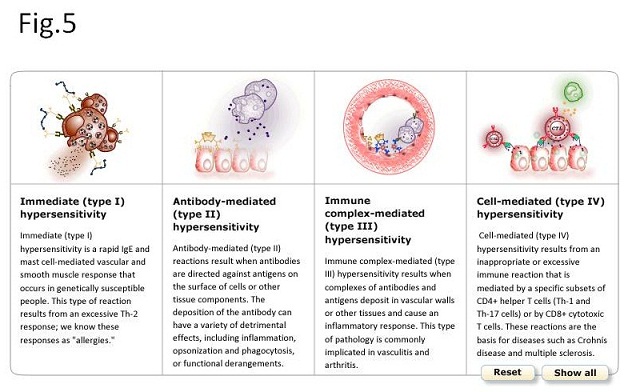
Hypersensitivity diseases are categorized into four groups; Immediate (type I) hypersensitivity related with mast cells, Ig E and histamine such as atopy, anaphylaxis and allergic rhinitis; Antibody (type II) mediated hypersensitivity such as rheumatic fever and Goodpasture syndrome; immune complex (of antigen and antibody, type III) mediated hypersensitivity such as SLE, MPO-ANKA and rheumatoid arthritis: T cell (type IV) mediated hypersensitivity such as acute hypersensitivity pneumonia, Crohn disease, and multiple sclerosis (2) (Fig. 5). Therefore, interstitial pneumonia observed in SLE occurs based on vasculitis of type III hypersensitivity disease. Clinically apparent interstitial lung disease (ILD) is less common in SLE since patients with long-standing disease are associated. Patients with long-standing disease more than 10 years of SLE onset are significantly more likely to develop clinical ILD (3). In our case, he had a long history of collagen disease. This time, clinically apparent dyspnea and low-level PO2 were manifested and chest CT showed compatible ILD that is currently referred as non-specific interstitial pneumonia (NSIP) but not usual interstitial pneumonia (UIP).
By definition, NSIP is one of idiopathic interstitial pneumonia which cannot be classified into usual interstitial pneumonia [UIP], acute interstitial pneumonia [AIP], desquamative interstitial pneumonia/respiratory bronchiolitis–associated interstitial lung disease [DIP/RB-ILD], organizing pneumonia [OP], lymphoid interstitial pneumonia [LIP] (4 – 6). OP is also a nonspecific pattern characterized by proliferation of fibrosis in the alveolar spaces and small airways associated with interstitial inflammatory infiltration. However, OP is limited to the local pulmonary area. As a result, NSIP implies a diagnosis of exclusion. NSIP is the most common manifestation of collagen vascular disease followed by exposure to various drugs (4 – 6). In our case, NSIP was associated with SLE.
Histologically, NSIP shows a non-unique uniform interstitial process with varying proportions of interstitial inflammation and fibrosis. Significant interstitial fibrosis is called fibrosing NSIP and cellular (mainly lymphocyte) infiltration to interstitial component is called cellular NSIP, inducing both types of NSIP expand interstitium, indicating the difficulty of radiological distinction (Figs 6, 7) (7, 8).
Meanwhile, NSIP is reported to precede prior to a SLE onset, implying radiological diagnosis of NSIP was important to check early SLE (3, 8). The most common radiologic features of NSIP (8, 9) are bilateral ground-glass opacities and fine reticulations (especially in fibrotic NSIP,) and pulmonary volume loss inducing traction bronchiectasis/bronchiolectasis. Areas of consolidation may be present. As opposed to UIP, honey comb pattern is usually absent, only found in advanced fibrotic NSIP. Subpleural sparing is considered very specific for NSIP (7-9). Minor subpleural reticulation is mainly found in fibrotic NSIP. However, the radiologic findings of NSIP are not sufficiently specific for definitive diagnosis. Confident diagnosis should be done based on clinical findings and compatible radiological findings. In our case, chest CT showed linear interstitial thickening and subpeural reticulation (Figs 1, 2)
Sialylated carbohydrate antigen KL-6 and surfactant protein D (SP-D) are produced by Type II alveolar cell. Active interstitial pneumonia induces vasculitis and hyperplasia and proliferation of Type II alveolar cell. KL-6 and SP-D move to blood from alveolar space due to higher penetration of vascular wall, leading to high values in interstitial pneumonia. SP-D elevates in various type pneumonia and KL-6 is more specific in interstitial pneumonia than SP-D (10). In our case, both values of KL-6 and SP-D were very high (KL-6: 3500 U/L, SP-D 219 ng/mL), indicating clinically active ILD.
NSIP respond well to corticosteroids and has a more favorable prognosis than UIP. Cessation of stimulating causes such as drugs and organ allergies are an imperative treatment strategy. In our case, high and tapering steroid therapy brought about improvement of dyspnea, decreasing KL-6 values.
【Summary】
We present a seventy three-year-old male with gradual worsening dyspnea and low-level PO2 with high level of KL-6 and SP-D indicating clinically apparent interstitial lung disease (ILD). He had a long history of collagen disease. CT showed non-specific interstitial pneumonia (NSIP) implying collagen vascular disease associated interstitial pneumonia. We should keep in mind that radiological findings of NISP opposed to usual interstitial pneumonia (UIP) were less honey comb pattern and subpleural sparing (subpleural minor reticulation). These findings reflect microscopic findings of interstitial edematous inflammation (cellular NSIP) and fibrosis (fibrosing NSIP). NSIP is the most common manifestation of collagen vascular disease followed by exposure to various drugs.


【References】
1.Mok, CC, et al. Pathogenesis of systemic lupus erythematosus. J Clin Pathol. 2003 Jul; 56(7): 481–490. PMCID: PMC1769989
2.Types of Hypersensitivity - Stomp On Step1 http://www.stomponstep1.com/hypersensitivity-type-1-2-3-4-urticaria-anaphylaxis
3.Mittoo S, Fischer A, Strand V, Meehan R, Swigris JJ. Systemic lupus erythematosus-related interstitial lung disease. Curr Rheumatol Rev 2010;6(2):99–107
4.Katzenstein AL, Fiorelli RF. Nonspecific interstitial pneumonia/fibrosis. Histologic features and clinical significance. Am J Surg Pathol. 1994 Feb. 18(2):136-47. [Medline].
5.American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am J Respir Crit Care Med. 2002 Jan 15. 165(2):277-304. [Medline].
6.Travis WD, et al. Idiopathic nonspecific interstitial pneumonia: report of an American Thoracic Society project. Am J Respir Crit Care Med. 2008 Jun 15. 177(12):1338-47. [Medline].
7.Akira M, et al. Usual interstitial pneumonia and nonspecific interstitial pneumonia with and without concurrent emphysema: thin-section CT findings. Radiology. 2009;251 (1): 271-9. doi:10.1148/radiol.2511080917 - Pubmed citation
8.Kim EA, et al. Interstitial lung diseases associated with collagen vascular diseases: radiologic and histopathologic findings. Radiographics. 2002;22 Spec No : S151-65. Radiographics (full text) - Pubmed citation
9.Mueller-mang C, et al. What every radiologist should know about idiopathic interstitial pneumonias. Radiographics. 27 (3): 595-615. doi:10.1148/rg.273065130 - Pubmed citation
10.Ohnishi H, et al. “Comparative study of KL-6, surfactant protein-A, surfactant protein-D, and monocyte chemoattractant protein-1 as serum markers for interstitial lung diseases”. Am. J. Respir. Crit. Care. Med. 2002;165: 378-81. PMID 11818324.
2017.9.27