

Clinical diagnosis
Case 8
【Progress】
After the second CT, she obtained drip infusion for dehydration and underwent emergent surgical laparotomy which revealed the necrotic small bowel stagnated with omental net adhesion. After surgical treatment, her symptoms and renal function improved dramatically. The patient was discharged 14 days after admission. Laboratory test at discharge; WBC 5420/ mm3; CRP 0.87 mg/dl; neutophils 79.5%. Creatinin 0.66 mg/dl, eGFR 65.4.
【Discussion】
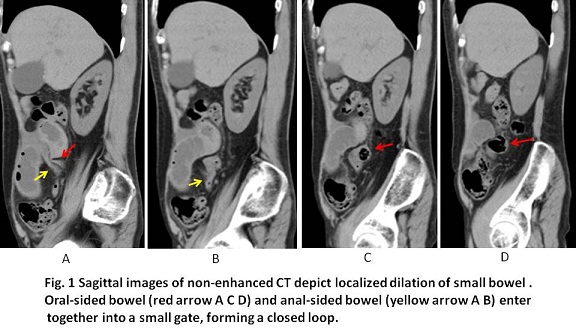
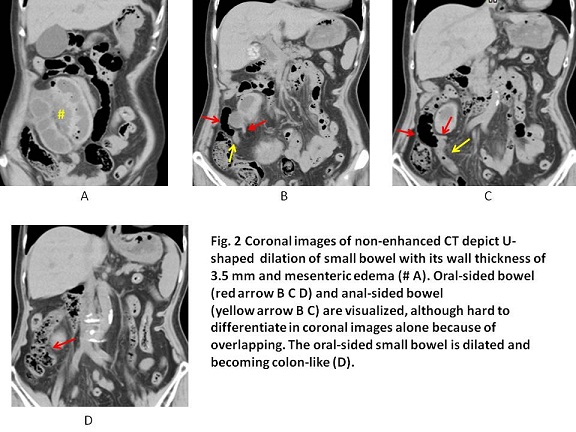
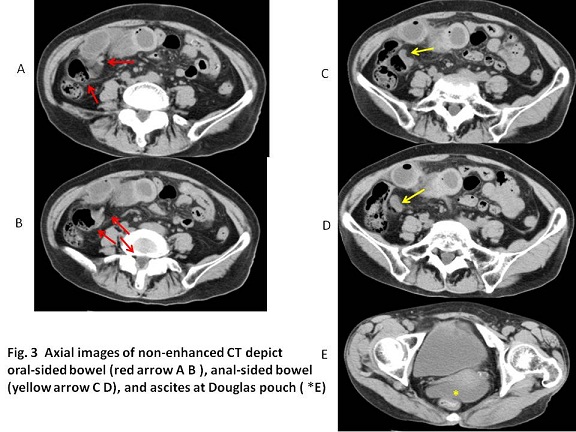
Whirl sign could not be detected in any CT image of axial, coronal and sagittal views of this case. Further, because of eGFR 15.0, contrast-enhanced CT was not conducted at day1. Then, we hesitated to give surgical laparotomy. However, the suspicious CT findings of the strangulation ileus which were listed in the previous literatures (1, 2, 3), were retrospectively found even in non-enhanced CT at day 1; beak sign; U shaped closed loop (radical distribution of mesenteric vessels); wall thickening of 2 mm or greater, mesenteric fluid (edema) inducing ascites. Beak sign of the anal-sided bowel at the transition site was clearly visualized rather than that of the oral-sided bowel in our case.
The mortality rates for non-gangrenous small bowel (SBV) obstruction range from 5.8% to 8%, while mortality rates for gangrenous SBV are higher, ranging from 20% to 100% (1, 4). Although our case discharged at day 14 without any complication, the speedy surgical procedure is preferable to avoid bowel resection.
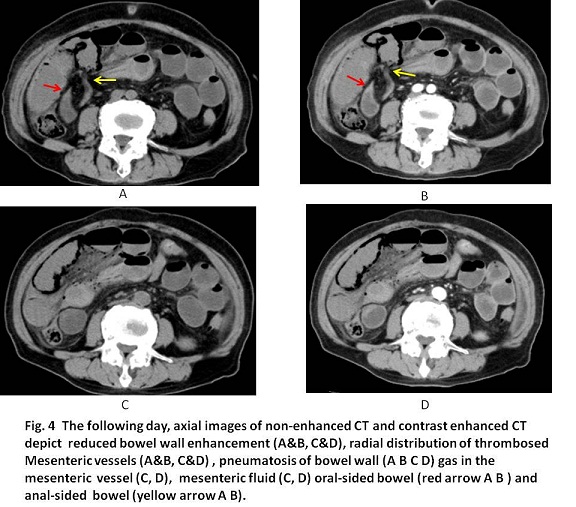
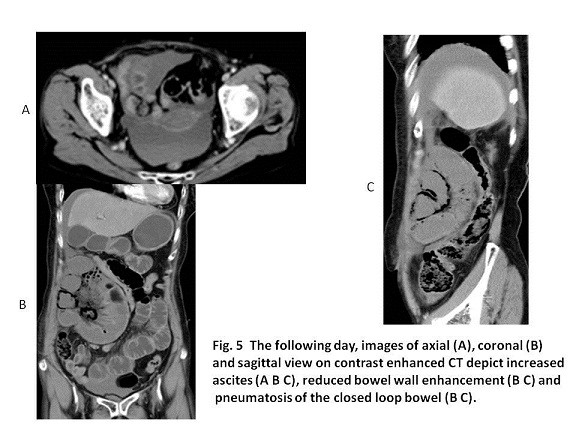
Adhesion is the most (80%) of the etiology of small bowel obstruction and as non-adhesive obstruction, cancer, hernia, gall stone and idiopathic volvulus are previously reported (1 2). In our case, CT at day 2 showed pneumatosis of the bowel wall, portal vein gas and reduced bowel wall enhancement, inducing to give the surgical resection of the necrotic bowel. Surgical laparotomy revealed an adhesion of string-like omentum which occurred after the previous appendectomy, causing the strangulation ileus.
It is reported that because the incidence of contrast induced nephropathy in patients with eGFR less than 30 is greater than 10% in large cohorts, contrast should not be administered (5, 6). Meanwhile, in patients with unstable renal function, an acute illness and/or acute renal failure, GFR calculation is reported to be unreliable (5, 6). In our case, although e-GFR was 15.0 at Day 2, the value of e-GFR was thought to be unreliable because of the acute onset of dehydration. Under the document of the referring attending physician saying the benefit of contrast overweighs the risk of contrast induced nephropathy, contrast-enhanced CT was conducted and surgical laparotomy was finalized under sufficient hydration, improving e-GFR of 65.4.
【Summary】
Non-enhanced CT in a seventy five-year-old female with a chief complaint of abdominal pain showed a closed loop sign, a beak sign, wall thickness of 3.5 mm and mesenteric edema, indicating strangulation ileus although whirl sign was not shown. Contrast-enhanced CT the following day, showed reduced bowel wall enhancement of closed loop, pneumatosis and portal vein gas. The patient received surgical resection of the necrotic bowel. The value of eGFR improved from 15.0 before contrast-enhanced CT to 65.4 after day 14 at discharge. The value of eGFR was unreliable for contrast induced nephropathy in this case because of acute dehydration.
【References】
1.Duda JB, Bhatt S, Dogra VS. Utility of CT whirl sign in guiding management of small-bowel obstruction. AJR Am J Roentgenol 2008;191:743-747.
2.Khurana B. The whirl sign. Radiology 2003:226:69-70.
3.Fisher JK. Computed tomographic diagnosis of volvulus in intestinal malrotation. Radiology 1981; 140:145-146.
4.Owuagwu O, et al. Small bowel volvulus: a review. J R Coll Surg Edinb 1999;44:150-155.
5.Guidelines for Intravenous Iodinated Contrast Administration in Outpatients Computed Tomography Examinations. https://radiology.ucsf.edu/patient-care/.../contrast/.../elevated-creatin.
6.Owen RJ et al. Consensus Guidelines for the Prevention of Contrast Induced Nephropathy. www.car.ca/.../standards%20guidelines/20110617_en_prevention
2016.06.01
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.