

Diagnosis
Case 96
【Progress】
Patients of Case 1 and 2 were treated by diuretics, and thereafter, their symptoms improved.
【Discussion】
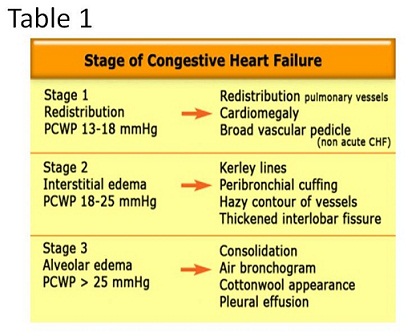
In the clinical reality, the differentiation using chest radiograph and chest CT between congestive heart failure (CHF) and acute respiratory distress syndrome (ARDS) is crucial. The differentiation is sometimes difficult and confusing. In the literature (1, 2), the image findings of CHF on chest radiograph change dependent on the stage; Stage I, cardiomegaly, vascular redistribution and broad vascular pedicle; Stage II, Karley B line, perivascular cuffing, hazy contour of vessels and thickened interlobular fissure; Stage III, pleural effusion, consolidation with air bronchogram and cotton wool appearance (Table 1). However, these typical findings do not always come out in the clinal cases but we encounter the equivocal lesion between CHF and ARDS.
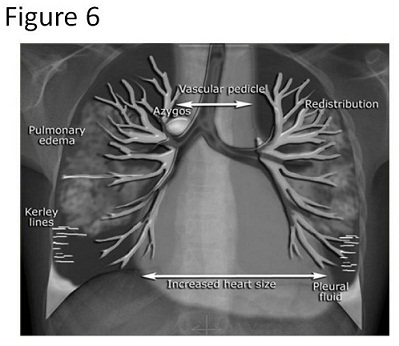
Vascular redistribution implies alteration of normal blood distribution. In the normal situation, the vessels in the upper lobe are smaller than the accompanying bronchus with a ratio of 0.85 (A3b / B3b). At the hilum level, they are equal. The vessels in the lower lobe are larger than the accompanying bronchus with a ratio of 1.35 (Fig. 6) (3, 4). There will be an increased artery-to-bronchus ratio in CHF. Further, the vascular pedicle indicates the distance between the right border of superior vena cava and the left border of the left subclavian artery. In the normal situation, a vascular pedicle width is less than 60 mm on a PA chest radiograph. That width more than 85 mm is pathologic (5). Both artery-to-bronchus ratio and vascular pedicle width are meaningful in erect PA chest radiograph but not in supine AP chest radiograph.
Expansion of azygos vein is third indicator of CHF. In the normal situation, the diameter of azygos vein is less than 5 mm in an erect AP position. Its diameter > 7 mm is most likely abnormal and a diameter > 10 mm is definitely abnormal. In a supine position, a diameter > 15 mm is abnormal (3 -6).
As the fourth indicator, haziness of pulmonary vessels is listed. In the normal situation, the margin of normal pulmonary vessels is clear, while in CHF, hazy and unclear margin of pulmonary vessels are found because of edema (6).
As the fifth indicator, thickness of interlobular fissure is listed (4 - 6). When chest CT is becoming to routinely conduct, this sign is probably most crucial of all the indicators. Interlobular fissure thickens because of fluid retention. Congestion of upper lobe gravitates to the fissure which means that the opacity of consolidation enhances intensely toward the interlobular fissure. This consolidation pattern is not found in cases with ARDS.
In our patients, pleural fluid and interlobular fissure effusion accompanied with pulmonary consolidation increased toward dorsally, in Case 1. and Case 2. Consolidation in the dorsal area of the right upper lobe was clearly bordered by the interlobular fissure, implying fluid retention gravitated to the dorsal and lower part. Whereas, in Cases 3-5, consolidation distributed to both lobes irrelevant to interlobular fissure, indicating no congestion of fluids.
【Summary】
We present chest CT images of five cases: two, cardiac failure; three, ARDS of anti-nuclear cytoplasmic antigen (ANCA), acute eosinophilic pneumonia and acute interstitial pneumonia. It is borne in mind that, in an erect PA chest radiograph, artery-to-bronchus ratio, vascular pedicle width, azygos vein diameter, presence or absence of haziness of pulmonary artery, and thickness of interlobular fissure are useful radiological findings indicative of CHF. However, in chest CT taken in supine position, interlobular fluid retention with gradual intense consolidation toward interlobular fissure is most crucial to differentiate CHF from ARDS.
【References】
1.Gluecker T, Capasso P, Schnyder P et-al. Clinical and radiologic features of pulmonary edema. Radiographics. 1999;19: 1507-31.
2.Cardinale L, Priola AM, Moretti F et-al. Effectiveness of chest radiography, lung ultrasound and thoracic computed tomography in the diagnosis of congestive heart failure. World J Radiol. 2014;6: 230-7.
3.Woodring JH. Pulmonary artery-bronchus ratios in patients with normal lungs, pulmonary vascular plethora, and congestive heart failure. Radiology, 1991;179:115-122.
4.Milne E, et al. The Radiologic Distinction of Cardiogenic and Noncardiogenic Edema (PDF). American Journal of Roentgenology, 1985;144: 879-894
5.Pistolesi M, et al. The vascular pedicle of the heart and the vena azygos. Part II: Acquired heart disease. Radiology 1984; 152: 9-17.
6.Harrison MO, et al. Radiological detection of clinically occult cardiac failure following myocardial infarction. Br J Radiol. 1971; 44:265-272
2018.3.14