

Clinical diagnosis
Case 3

【Progress】
At first, radiofrequency ablation for treatment was considered to attempt. However, because of the tumor composing of the hard component and situating beneath liver capsule, the patient underwent surgical wedge resection. A microscopic finding of the specimen revealed viable tumor in the surrounding and massive fibrosis with necrosis at the center corresponding to the hyperintence and the hypointence component, respectively. Histological diagnosis was cholangiocarcinoma.
【Discussion】
The histology of peripheral intrahepatic cholangiocarcinoma (PIH) is basically adenocarcinoma. In these days, PIH is reported to include the resemblance components originated from hepatic cells, cholangiocells and Hering ducts (1,2). As well-known, there exists a mixed carcinoma of hepatocellular carcinoma and cholangiocarcinoma (1). The configuration and pathology of PIH are possibly colorful because of the genesis from pleural genetic processes or from hepatic stem cells (1, 2). PIH is well-known to occur from chronic biliary tract disorder (1). The incidence of PIH occurrence from chronic hepatic disorder is recently reported to increase (1, 2). In this case, hepatocellular carcinoma, first, occurred and approximately five years later, PIH followed.
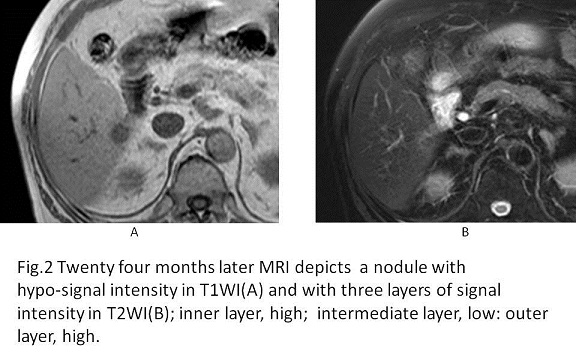
Kim et al. classified mass-forming PIHs on dynamic MRI using EOB into a typical hyper-intense type and an atypical( hyper- and hypo- intense) type (3). The hypo-intense area of the atypical type situated in the center was gradually enhanced on a hepatic cell phase, which might not be pathognomonic because of difficulty differentiation between cholangiocarcinoma and hepatic colorectal metastasis; however, this finding, which reflected severe fibrosis, appears to be one of the characteristic markers of PIH (3-5)
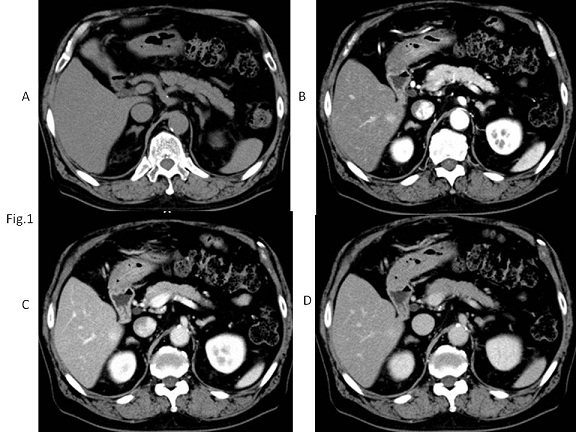
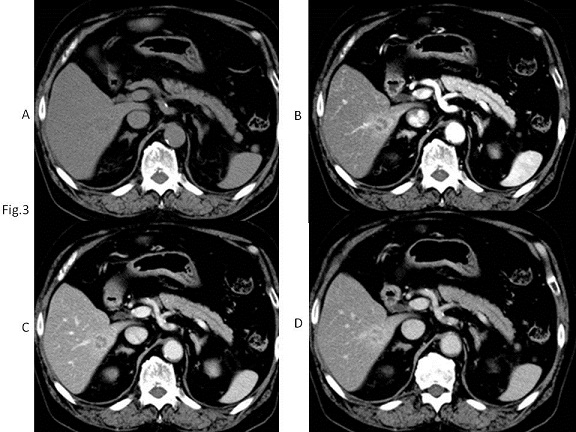
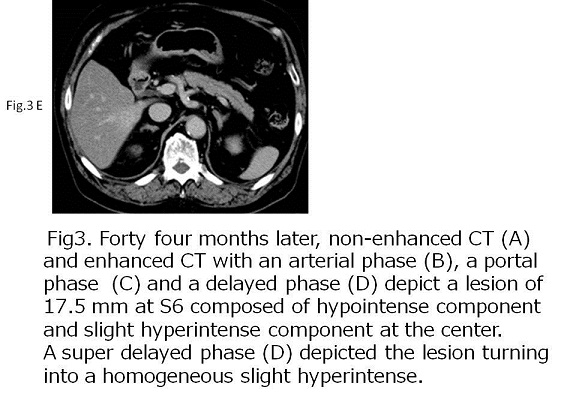
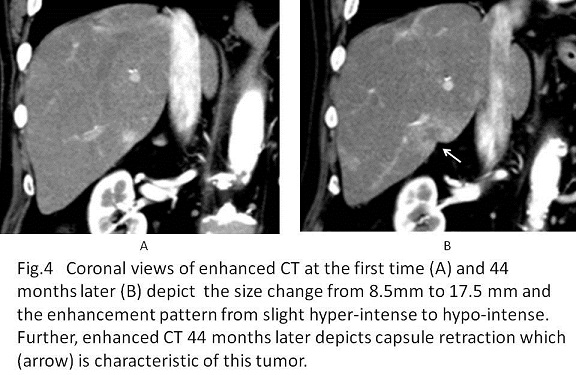
On enhanced CT images at the initial stage of our case, the tumor had the hyper-intense density in an arterial phase, decreasing the density into the iso-intense density in a delayed phase. Meanwhile, on enhanced CT 44months later, the tumor had the mixed intense density of hyperintense and hypointense. The central hypointense area was gradually enhanced, leading to the iso-intense in a super-delayed phase.
The presence of intrahepatic bile duct dilatation may indicate cholangiocarcinoma (1, 2). However, PIH does not always occur with intrahepatic bile duct dilatation in case of occurrence at the site beneath liver capsule (1-5). Instead, capsular retraction on CT or MRI images is sometimes encountered due to fibrous proliferation of the tumor (3-5). In the clinical process of this case, no bile duct dilatation was observed. However, the capsular retraction appeared on the CT scanned forty four months after, although it did not appear on CT at the initial stage.
【Summary】
A seventy four-year-old male had a small PIH five years after he had received hepatic sub-segmentectomy for hepatocellular carcinoma. Contrast enhanced CT at the initial stage depicted the small hyperintense tumor. Thereafter, the tumor grew with the hyperintense component in the surrounding and the hypointense component in the center, and the capsular retraction. Histological examination revealed the fibrosis and necrosis corresponded to the hypotense component and viable tumors corresponded to the hypertense component. The central hypointense area with the gradual enhancement and the capsular retraction on contrast-enhanced CT might help clinicians help to diagnose PIH.
【References】
1.Shimonishi T,et al. Histolpgic features of intrahepatic cholangiocarcinoma. The Biliary tract & pancreas. 1997; 18: 1085-1090
2.Sanada Y, et al. Review to better understand the macroscopic subtypes and histogenesis of intrahepatic cholangiocarcinoma.World J Gastrointest Pathophysiol. 2014; 5: 188–199.
3.Kim SH, et al. Typical and atypical imaging findings of intrahepatic cholangiocarcinoma using gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging. J Comput Assist Tomogr. 2012;36:704–709.
4.Nanashima A, et al. Intrahepatic cholangiocarcinoma: relationship between tumor imaging enhancement by measuring attenuation and clinicopathologic characteristics. Abdom Imaging. 2013;38:785–792
5.Kang Y, et al. Intrahepatic mass-forming cholangiocarcinoma: enhancement patterns on gadoxetic acid-enhanced MR images. Radiology. 2012;264:751–760.
2016.04.20
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.