

Clinical diagnosis
Case 30
Punctured plural fluid was unclear reddish fluids including sediments: the number of cells 3150/mm3, neutrophils 92%, sugar 108mg/dL, protein 5.7g/dL. He underwent percutaneous catheter drainage targeting the large abscess in the right central area via the intrapulmonary route. This management caused pneumothorax as one of the major complication. The drainage catheter was re-inserted and placed to pleural space for drainage under CT guidance and persistent air absorption was conducted for maintaining negative pressure. Regrettably, 10 days later, he passed away because of sepsis and poor pulmonary function.
【Discussion】
Radiographic findings of chest radiograph between pyothorax (empyema) and lung abscess are sometimes similar: cavities with air fluid level (1). The differentiation between pyothorax and lung abscess is imperative because of the evaluation of treatment strategy (2).
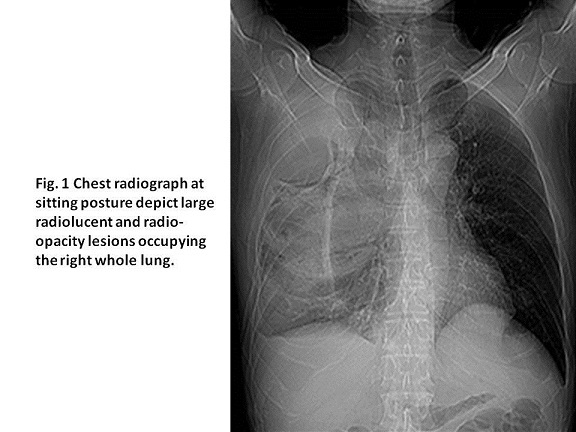
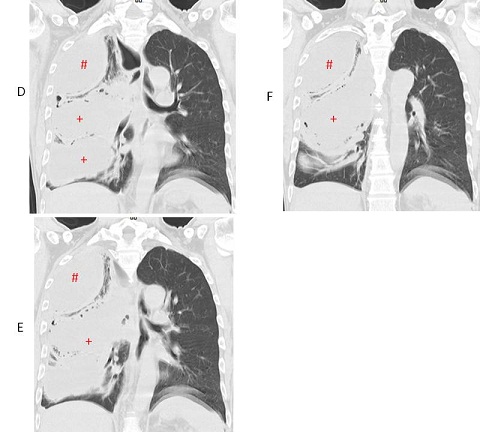
The pleural space is reported normally filled with 5 to 10 mL of serous fluid, which is secreted mainly from the parietal pleura and absorbed through the lymphatics in the parietal pleura (3, 4). The imbalance between the secretion and absorption causes macroscopic accumulation of pleural effusion. In the clinical situation, congestive heart failure, pneumonia and malignancy are the most common causes of pleural effusions (3-5). Pyothorax is a collection of purulent fluid in the pleural space. The most common cause of pyothorax is pneumonia (parapneumonic pleural effusion) (3-12). In our case, Fig 1G showed small pneumonia in the right lower lobe which is the suspicious trigger of pyothorax. In short, pneumonia inflates to the intralobar pleural space (minor fissure), the pleural effusion becomes infected and neutrophils buildup, inducing pyothorax. Although the distribution of causative organisms does differ greatly in adults, it is reported that in an analysis of children, streptococcus pneumoniae is the most in 51% followed by streptococcus pyogenes in 9% and staphylococcus aureus in 8%(6). Percutaneous drainage is targeting the first therapeutic management with the success rate of more than 90% (3-13). In our adult case, the pleural fluid culture found no organism.
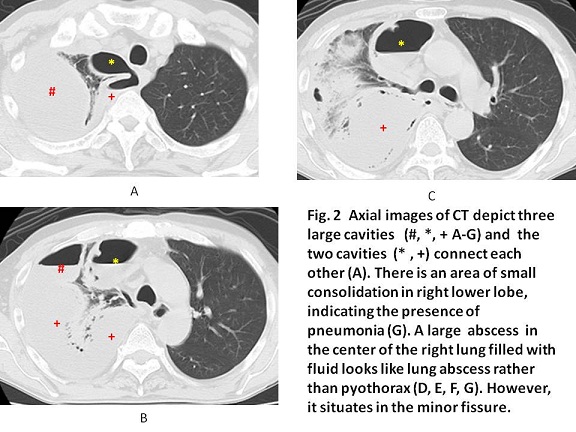
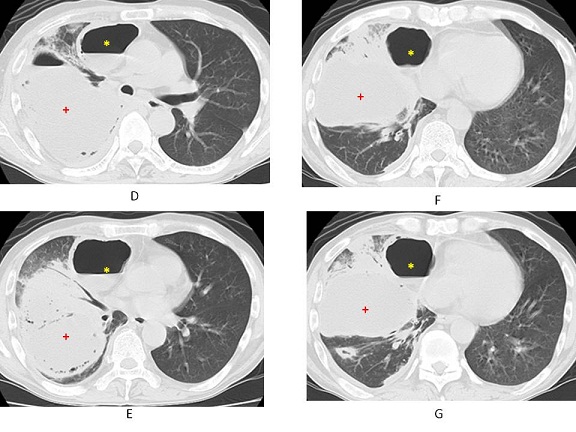
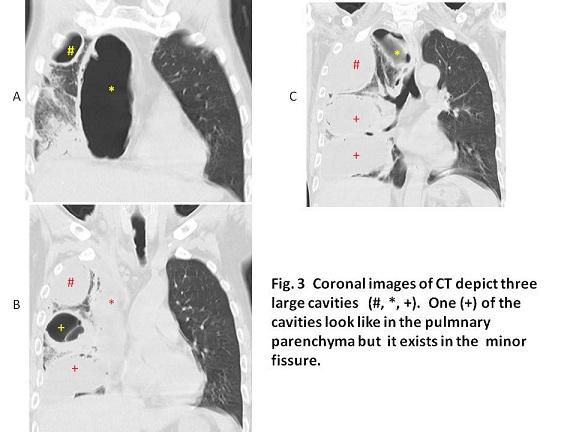
In our case,a large pyothorax in the minor fissure resembled a lung abscess. A lung abscess is caused by an aspiration of bacteria-containing oropharyngeal secretions which induce necrosis and cavities in the pulmonary parenchyma (14-16). Anaerobic mouth flora is the most common organism in a primary lung abscess (14-16). It more often involves the right lung than the left (16). Lung abscesses are most commonly managed by medical treatment with prolonged antibiotics. However, medical treatment can be failed if the patient has poor prognostic factors, such as a large abscess cavity (> 6 cm) (16). Eleven to 21% of patients with lung abscesses eventually require surgical or percutaneous drainage due to antibiotics treatment failure (16). The success rate of CT-guided drainage of a lung abscess is up to 90% (14-16). Pneumothorax is one of the complications (14-16).
CT-guided percutaneous drainage irrespective of a pyothorax or a lung abscess should be considered as the initial treatment of choice (3- 11, 13-16). In our case, the catheter drainage was initially tried targeting the large abscess in the right central pulmonary area which was at first thought to be a large lung abscess. The catheter drainage was conducted via the pulmonary parenchyma, inducing pneumothorax. It was considered retrospectively that the central large abscess was a part of the pyothorax in the intrapleural space (minor fissure). The catheter puncture route for pleural space avoiding the pulmonary parenchyma was possible. As a result, pneumothorax caused the delay of pulmonary function recovery, regrettably inducing the fatal sepsis.
【Summary】
We present a fifty one-year-old male with pyothorax. A chest radiograph and CT showed cavities formation similar findings as lung abscess. A drainage catheter insertion was conducted, targeting the large abscess via the pulmonary parenchyma. It caused pneumothorax. However, in retrospect, that large abscess probably situated intrapulmonary pleural space (minor fissure). Puncturing the pleural space directly without the route of pulmonary parenchyma might prevent the complication of pneumothorax and protect the pulmonary function. The patient passed away because of sepsis. The appropriate diagnosis and safety management of the percutaneous catheter drainage under CT guidance are crucial to evaluate the appropriate route for the pyothorax.
【References】
1.Stark D D, et al. Differentiating lung abscess and empyema: radiography and computed tomography. AJR Am J Roentgenol. 1983;141(1):163–167.
2.Hyeon Yu. Management of Pleural Effusion, Empyema, and Lung Abscess. Semin Intervent Radiol. 2011 Mar; 28(1): 75–86. doi: 10.1055/s-0031-1273942
3.Chung J, et al. Pleural effusion and empyema thoracis. In: Bope E T, Rakel R E, Kellerman R D, editors. Conn's Current Therapy 2010. 1st ed. Philadelphia: Saunders/ Elsevier; 2010. pp. 263–265.
4.Bouros D, et al. Parapneumonic effusion and empyema: best therapeutic approach. Monaldi Arch Chest Dis. 2001;56(2):144–148.
5.Schiza S, et al. Clinical presentation and management of empyema, lung abscess and pleural effusion. Curr Opin Pulm Med. 2006;12(3):205–211.
6.Byington CL, et al. "An epidemiological investigation of a sustained high rate of pediatric parapneumonic empyema: risk factors and microbiological associations". Clinical Infectious Diseases. 2002: 34: 434–40. doi:10.1086/338460
7.Light R W. Parapneumonic effusions and empyema. Clin Chest Med. 1985;6(1):55–62.
8.Keeling A N, et al. Empyema and effusion: outcome of image-guided small-bore catheter drainage. Cardiovasc Intervent Radiol. 2008;31(1):135–141.
9.Light R W, et al. Management of parapneumonic effusions. Clin Chest Med.1998;19(2):373–382.
10.Moulton J S. Image-guided management of complicated pleural fluid collections. Radiol Clin North Am. 2000;38(2):345–374.
11.Light R W. Clinical practice. Pleural effusion. N Engl J Med. 2002;346(25):1971–1977.
12.Pierrepoint M J, et al. Pigtail catheter drain in the treatment of empyema thoracis. Arch Dis Child. 2002;87(4):331–332.
13.Alfageme I, Munoz F, Pena N, Umbria S (1993). "Empyema of the thorax in adults. Etiology, microbiologic findings, and management". Chest. 103 (3): 839–43. doi:10.1378/chest.103.3.839.
14.Morrow L E, et al. Primary Lung Abscess. In: Bope E T, Rakel R E, Kellerman R D, editors.Conn's Current Therapy 2010. 1st ed. Philadelphia: Saunders/Elsevier; 2010. pp. 266–267.
15.Mwandumba H C, et al. Pyogenic lung infections: factors for predicting clinical outcome of lung abscess and thoracic empyema. Curr Opin Pulm Med. 2000;6(3):234–239
16.Davies C W, et al. Pleural Diseases Group, Standards of Care Committee, British Thoracic Society BTS guidelines for the management of pleural infection. Thorax. 2003;58 (Suppl 2):ii18–ii28.
2016.11.2
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.