

Clinical diagnosis
Case 38
The pain relief was obtained by Tegretol and the gradual decrease of the dosage was scheduled. If the decrease trial were not effective, he would consult with neurosurgeon.
【Discussion】
The trigeminal nerve is the fifth cranial nerve and the largest of the twelve cranial nerves. It comes out of the superior-lateral aspect of pons (1). It includes three branches: ophthalmic, maxillary and mandibular branch nerves. The ophthalmic and maxillary nerves are purely sensory and the mandibular nerve has sensory and motor functions. The motor branch of the mandibular nerve controls the mastication muscles. The trigeminal nerve comes out of the lateral aspect of the upper pons and enters Meckel cave via the prepontine cistern, forming the semilunar ganglion (1).
Trigeminal neuralgia is estimated occur with the annual incidence of 0.4-2 per 10,000 people and usually begins in people over 50 years old, with prevalence increasing with age (2-4). The maxillary branch is the most affected and the ophthalmic branch the least. Women are more affected than man (1.5 vs 1) (2-4). Trigeminal nerve delivers feelings of the face and surface of the eye. Trigeminal neuralgia usually causes severe facial pain that lasts for a few seconds on the side of the affected nerve, in some cases the pain can last for minutes to hours and even become constant (2-4). In our case aged 61 male, trigeminal neuralgia underneath ear from the maxillary branch suddenly occurred for a few second two weeks ago and then, became constant since last night. The area surrounding eye from the ophthalmic branch became most painful.
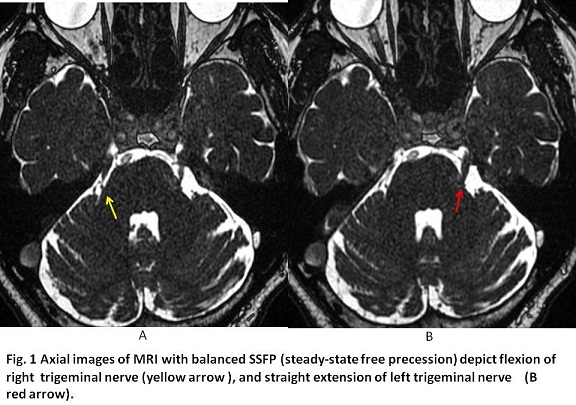
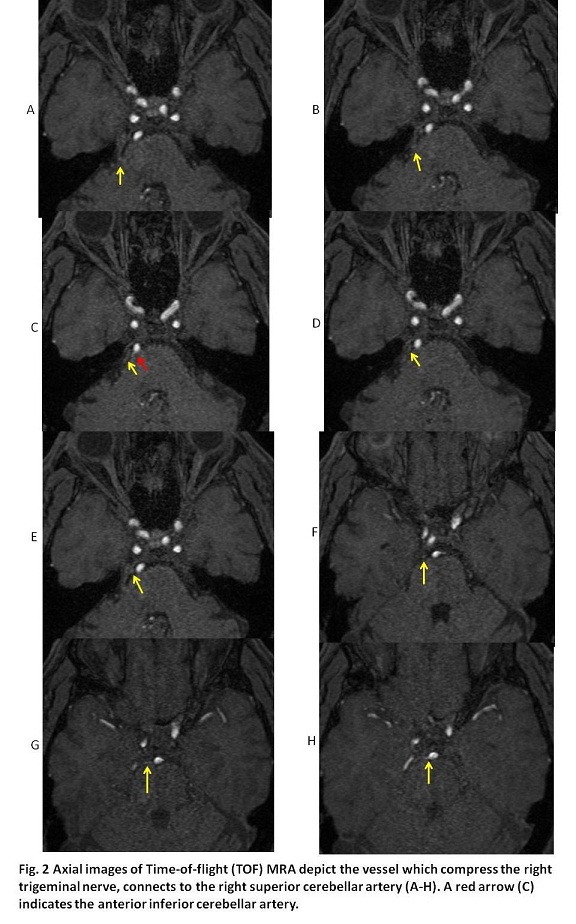
Trigeminal neuralgia is believed to be mainly caused by a blood vessel pressing on the trigeminal nerve at its exit portion from the pons (5-7). It can occur in patients with multiple sclerosis and cranial tumor compression (6, 7). The responsible artery is most commonly the superior cerebral artery (5-7). Middle brain is blood-supplied by posterior cerebral artery and superior cerebellar artery, pons by basilar artery rami and medulla oblongata by anterior cerebellar artery, posterior cerebellar artery and anterior spinal artery. Further, superior cerebellar artery transverses upper part of the pons, anterior inferior cerebellar artery transverses between pons and medulla oblongata and posterior inferior cerebellar artery transverses the lower part of medulla oblongata (1). The trigeminal nerve comes out of pons and the superior cerebellar artery arises near the termination of the basilar artery and runs near trigeminal nerve (1). In our case, compared MRI with time of flight and with balanced SSFP (steady-state free precession) (5), lengthened loop branch of the superior cerebellar artery was confirmed to compress the right trigeminal nerve at its exit from pons. Persistent compression can injure the local myeline sheath and cause irritating and hyperactive function of the 5th cranial nerve, possibly falling into demyelination of axon.
The initial treatment for trigeminal neuralgia is medication with Tegretol (carbamazepine) (2-4, 8). In case of being non-effective, microvascular decompression is supplied, relocating or removing blood vessels that are in contact with the trigeminal nerve and placing a pad between the nerve and arteries (2, 8). Microvascular decompression of the trigeminal nerve root is regarded as an efficient and durable treatment (8). Herpes zoster often affects trigeminal nerves, most ophthalmic branch nerve which is the result of reactivation of herpes zoster that remained dormant in the trigeminal nerve root or ganglion following infection of chickenpox in children (9). In our case, herpes zoster was deniable because of no skin rash. Tegretol seems to be quite effective on pain relief and then, microvascular decompression is not scheduled at present.
【Summary】
We present a sixty one-year-old male suffering from right facial throbbing pain. MRI with time of flight and MRI with balanced SSFP showed the flexion of right trigeminal nerve due to the compression of superior cerebellar artery. We should keep in mind that the elongated branch of superior cerebellar artery is the most to cause the compression of the trigeminal nerve whose myelin sheath is injured, causing irritation and hyperactivity of the trigeminal nerve.
【References】
1.Peter Duus. Neuroloigisch-topische Diagnostik: Anatomie Physiologie Klinik, second edition translated in Japanese by Hajime Handa and Junya Hanakita. Bunkodo, Tokyo
2.Nurmikko, TJ, et al. Trigeminal neuralgia—pathophysiology, diagnosis and current treatment. Pain; 2009 :87: 165–166.
3.Krafft RM. Trigeminal neuralgia. Am Fam Physician. 2008;77 : 1291-1296. Pubmed citation
4.Zakrzewska JM, et al. Trigeminal neuralgia. BMJ. 2014;348 (feb17 9): g474. doi:10.1136/bmj.g474 - Pubmed citation
5.Prieto R, et al. Trigeminal neuralgia: Assessment of neurovascular decompression by 3D fast imaging employing steady-state acquisition and 3D time of flight multiple overlapping thin slab acquisition magnetic resonance imaging. Surg Neurol Int. 2012;3 (1): 50. doi:10.4103/2152-7806.96073 - Free text at pubmed - Pubmed citation
6.Tash RR, et al. Trigeminal neuralgia: MR imaging features. Radiology. 1989;172 (3): 767-70. doi:10.1148/radiology.172.3.2772186 - Pubmed citation
7.Hughes MA, et al. MRI of the Trigeminal Nerve in Patients With Trigeminal Neuralgia Secondary to Vascular Compression. AJR Am J Roentgenol. 2016;206 : 595-600. doi:10.2214/AJR.14.14156 - Pubmed citation
8.Gronseth G, et-al. Practice parameter: the diagnostic evaluation and treatment of trigeminal neuralgia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies. Neurology. 2008;71 (15): 1183-90. doi:10.1212/01.wnl.0000326598.83183.04 - Pubmed citation
9.Carbone V, et al. Herpes zoster of the trigeminal nerve: a case report and review of the literature. Minerva Stomatol. 2004;53:49-59
2016.12.28
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.