

Clinical diagnosis
Case 44
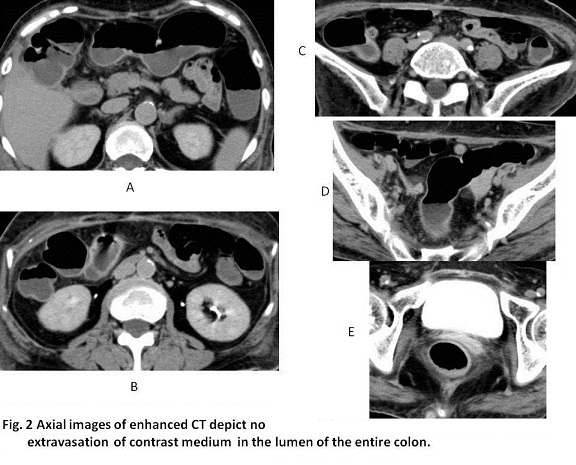
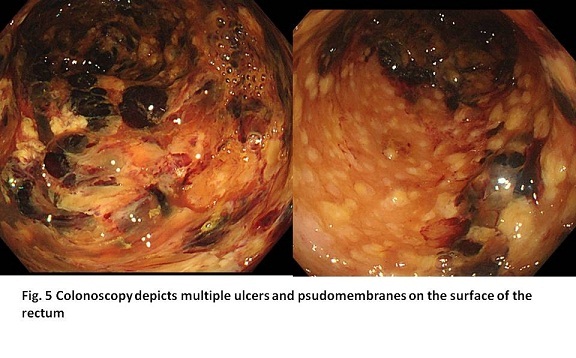
Colon endoscopy revealed multiple ulcers and pseudomembrane on the surface of rectum and sigmoid colon (Fig. 5). Stool culture detected Clostridium difficile. Enhanced CT depicted no extravasation of contrast medium (Figs 2, 3, 4), which might be not for good timing for detecting bleeding. The marked decrease of Hb values from 8.6g/dL to 4.3g/dL urged us to conduct angiography, but it did not show no detection of bleeding sites . Venous transfusion of red blood cells elevated hemoglobin of 7.9 g/dL. Regrettably, two weeks later, she passed away due to tumor increase and colon dysfunction.
【Discussion】
A healthy colon is in a good balance of normal flora. The use of antibiotics or other drugs such as anticancer drugs induces to break the healthy balance, causing drug-induced colitis, resulting from the bacterial production of toxins. In other words, not merely antibiotics such as penicillins, cephalosporin and clindamycin but also chemotherapy disrupt the normal flora (1-7). Pseudomembranous colitis is mainly caused by toxins produced by Clostridium difficile, a gram-positive anaerobic bacillus. Stool culture is evaluated to be the most sensitivity test: sensitivity 90-100%, specificity 84-100% (1-7). In our case, the first stool culture was positive but the second one was negative.
The toxins attack the mucosal layers, resulting in cytoplasmic contraction of mucosal cells, hemorrhage, inflammation, cellular necrosis and protein loss. Further, they increase capillary permeability and peristalsis, inciting diarrhea and bleeding. Psudomembrane is pathologically formed by necrotic mucoepithelial cells, muscus, fibrin and neutrophils. The main predisposing area is mucoepithelial sub-layer of the mucosal layer. Basically, the layers of mucosal muscularis, submucosa and smooth muscularis are not involved. The mucoepithelial sublayer of the entire colon was disrupted, inducing toxic megacolon. In our case, psudomembrane colitis was found in the entire colon, inducing fatal colon dysfunction.
Although not so often, pseudomembrane colitis is reported to be caused by the other etiology rather than Clostridium difficile such as infectious colitis of Campylobacter, cytomegalovirus, Escherichia coli 0157, Salmonella, and ischemic colitis by occlusive mesenteric arteries (9-12).
Pseudomembranous colitis is categorized in three degrees of mild, moderate and severe; mild, diarrhea only; moderate, diarrhea without symptoms/signs meeting the definition of severe; severe, hypoalbuminemia (serum albumin < 3g/dL) and either a white blood cell count ≥15,000 cells/mm3 or tenderness (1-5). Complicated Clostridium difficile infection is added in case of admission of intensive care unit with hypotension, fever 38.5 °C, significant abdominal distension, mental status change, or WBC ≥35,000 cells/mm3 or <2,000 cells/mm3(1-5). As treatment, metronizadole and/or vancomycin are used and its doses are adjusted dependent upon the criteria of severity.
In the mild or moderate degrees, pseudomembrane colitis does not always affect the whole colon. In the localized cases, psudomembranous colitis is limited to the cecum and the proximal colon (with the incidence of 5-15%) (1-5). Grossly bloody stools are also unusual in mild degree and moderate degree (1-6).
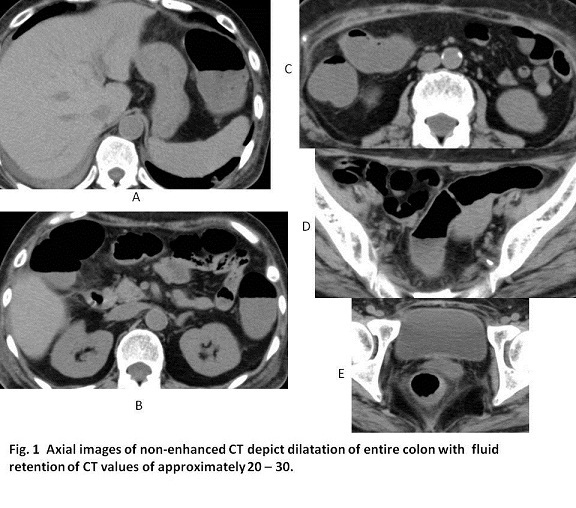
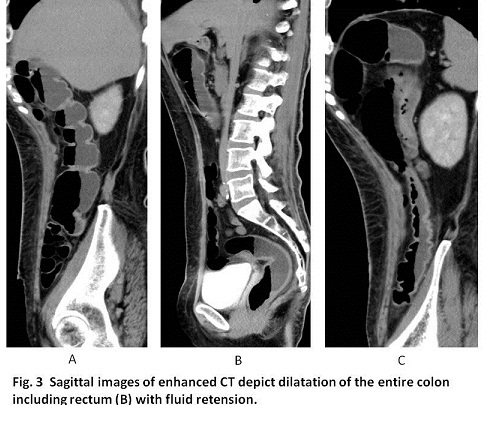
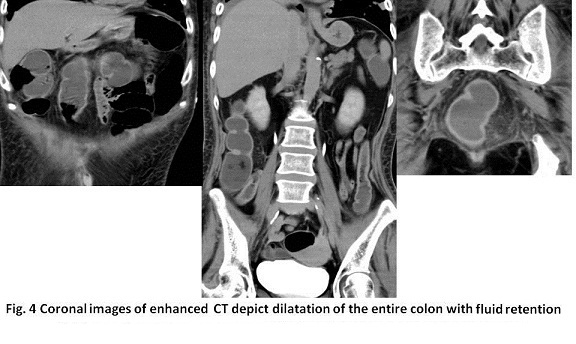
In our case, anticancer drugs for recurrent gingival cancer caused pseudomembranous colitis in the entire colon with severe diarrhea and massive bleeding. Non-enhanced CT depicted dilatation of the entire colon with bloody fluid retention of CT values of approximately 30, indicating the category of complicated clostridium defficile infection. Contrast-enhanced CT and angiopraphy of superior mesenteric artery and inferior mesenteric artery did not show the bleeding sites, indicating bloody stool did not result from arterial bleeding but probably capillary hemorrhage.
【Summary】
We present a case with pseudomembrane colitis with colon bleeding caused by chemotherapy for recurrent gingival cancer. Colonoscopy depicted pseudomembrane and multiple ulcers. CT depicted the dilatation of the entire colon with bloody fluid, indicating the category of complicated Clostridium difficile infection. Colon bleeding in our case is unusual and fatal. The mucoepithelial sub-layer of the mucosal layer falls in necrosis forming peudomembrane with fibrin, muscus and inflammatory cells. When these changes prevails the entire colon, the poor prognosis is possible. We should keep in mind that there exists the degree category of Clostridium defficile infection and in mild and moderate degree, the cecum and the proximal ascending colon are predisposing sites, while in severe degree, the entire colon is susceptible, possibly falling in fatal prognosis. The speedy treatment of using metronidazole and/or vancomycin is necessary to interrupt severe degree.
【References】
1.Gujja D, et al. Predictors of serious complications due to Clostridium difficile infection. Aliment Pharmacol Ther 2009;29:635–642.
2.Fujitani S, et al. Comparison of clinical severity score indices for Clostridium difficile infection. Infect Control Hosp Epidemiol 2011;32.
3.Dudukgian H, et al. Clostridium difficile colitis—predictors of fatal outcome. J Gastrointest Surg 2010;14:315–322.
4.Byrn JC, et al. Predictors of mortality after colectomy for fulminant Clostridium difficile colitis. Arch Surg 2008;143:150–154
5.Sailhamer EA, et al. Fulminant Clostridium difficile colitis: patterns of care and predictors of mortality. Arch Surg 2009;144:433–439; discussion 439–40.
6.Pepin J, et al. Risk factors for mortality following emergency colectomy for fulminant Clostridium difficile infection. Dis Colon Rectum 2009;52:400–405.
7.Bhangu S, et al. Mortality and risk stratification in patients with Clostridium difficile-associated diarrhoea. Colorectal Dis 2010;12:241–246.
8.Lungulescu OA, et al. CSI: a severity index for Clostridium difficile infection at the time of admission. J Hosp Infect 2011;79:151–154.
9.C. R. Dignan, et al. Can ischemic colitis be differentiated from C difficile colitis in biopsy specimens? The American Journal of Surgical Pathology, vol. 21, no. 6, pp. 706–710, 1997. View at Publisher • View at Google Scholar • View at Scopus
10.Villanacci, S, et al., “Pseudomembranous collagenous colitis with superimposed drug damage,” Pathology—Research and Practice, vol. 209, no. 11, pp. 735–739, 2013. View at Google Scholar
11.A. Uc, F, et al. Pseudomembranous colitis with Escherichia coli O157:H7. Journal of Pediatric Gastroenterology and Nutrition, vol. 24, no. 5, pp. 590–593, 1997. View at Publisher • View at Google Scholar • View at Scopus
12.Surawicz CM, et al. Pseudomembranous colitis: causes and cures. Digestion; 60, 91–100, 1999.
2017.3.1
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.