

Clinical diagnosis
Case 64
【Progress】The infant was transported to the specialized children hospital where she previously received surgical management for diaphragmatic hernia. Approximately two months later, they reported us about the progress including treatment process as below.
Ileus tube was first inserted to the bowel, which brought a relief of ischemic symptoms. However, no stool was found for a week, indicating the limit of ileus tube management. Then, peritoneal endoscopic ileus-releasing management was first conducted. Endoscopic diagnosis was Meckel diverticulum torsion. Under endoscopic control, the wedge resection of the small bowel was performed to relieve from tightly adhesive connective tissue. After the management, bowel gas was moving to the anal side but stool evacuation was not found yet. Then, open surgery was finally conducted which revealed two tightly adhesions, causing complete closure of lumen and partial bowel necrosis. As a result, she received open partial resection and reconstructive end-to-end anastomosis of small bowel. The final diagnosis was ileus due to adhesion. Two weeks later, she was discharged in a healthy condition.
【Discussion】
Intestinal obstruction in the newborn is caused by atresia of digestive organs. Intestinal obstruction in the infants aged 3 months to 6 years is caused mostly by intussusceptions followed by incarcerated inguinal hernia and bowel malrotation (1-3). Although the cause of intussusceptions is not clarified, a virus infection such as adenovirus or rotavirus is suspected because of the seasonal predisposition (4–7). The swollen lymphoid adenopathy such as Peyer’s patch or localized swollen bowel wall by virus infection might become the leading point of intussusceptions. Meckel diverticulum, inflammatory polyp and duplication cyst can be also the leading point.
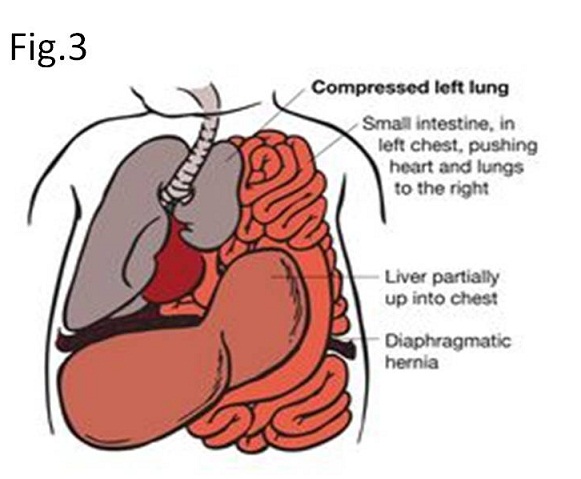
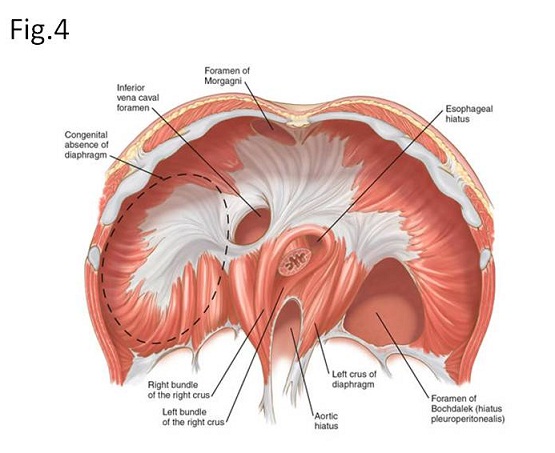
Congenital diaphragmatic hernia occurs 1 in 2000 to 2500 births (Fig. 3)(8-11). It causes pulmonary hypertension and pulmonary hypoplasia. A left-sided Bochdalek hernia occurs in approximately 85% and a right sided Bochdalek henia does in approximately 13%. Anterior Morgani hernia represents approximately 3% (8-11)(Fig. 4). Most fetuses with congenital diaphragmatic hernia are stillborn and even if survived, the mortality of newborns is still high. Surgical management consists of replacing the digestive organs into the abdominal cavity and primary or patch closure for diaphragmatic defect.
Postoperative adhesion is one of a major cause of small bowel occlusion (12). Because no resection of small bowel was conducted for repair of diaphragmatic hernia, adhesive occlusion seems likely not to occur. The pediatric surgeon who supplied surgical managements in our case explained us as follows; because the abdominal cavity with congenital diaphragmatic hernia was relatively narrow compared with the healthy abdominal cavity, the herniated digestive organ had to be compelled to force into the narrow abdominal cavity: it might cause small bowels abruptly bend and fold, inducing the adhesion between bowel and bowel and between bowel and abdominal wall and leading to adhesive ileus.
During laparascopic management in our case, Meckel diverticulum was considered to relate with adhesive ileus such as mesodiverticular band. According to Rutherford et al., ileus is caused by Meckel diverticulum under the following situation (13): diverticulum torsion, interssuception, mesodiverticular band (remnant of the vitelline vessel nourished on yolk duct) and inverted diverticulum. However laparotomy conducted after laparoscopy revealed absence of Meckel diverticulum but presence of adhesive ileus with partial necrosis of small bowel.
【Summary】
We present a three years and three-month-old infant suffering from abdominal pain, vomiting and fever. She had experienced surgical management for diaphragmatic hernia soon after birth. This time, the infant experienced laparotomy following insertion of ileus tube, which revealed adhesive ileus with partial necrosis of small bowel. We should keep in mind that abdominal cavity is narrow in diaphragmatic hernia compared to that in healthy abdominal cavity and the management of forcing herniated small bowel into the narrow abdominal cavity results in abruptly bending and folding of small bowels, leading to adhesive ileus. Further, in case of no history of surgical management, small bowel obstruction mostly occurs in intussusceptions followed by incarcerated inguinal hernia, bowel malrotation and Meckel diverticulum-related disease.

【References】
1.Kitagawa S., Miqdady M. Intussusception in children. UpToDate. 2014; Accessed: October 2015.
2.Mansour AM, et al. Enteric viral infections as potential risk factors for intussusception. J Infect Dev Ctries. 2013 Jan. 7(1):28-35. [Medline].
3.Nylund CM, et al. Bacterial enteritis as a risk factor for childhood intussusception: a retrospective cohort study. J Pediatr. 2010 May. 156(5):761-5. [Medline].
4.Weintraub ES, et al. Risk of intussusception after monovalent rotavirus vaccination. N Engl J Med. 2014 Feb 6. 370(6):513-9. [Medline].
5.Patel MM, et al. Intussusception risk and health benefits of rotavirus vaccination in Mexico and Brazil. N Engl J Med. 2011 Jun 16. 364(24):2283-92. [Medline].
6.Manish M. Et al. Intussusception risk and healt benefits of rotavirus vaccination in Mexico and Brazil. The New England Journal of Medicine. Jun 2011. 364 (24):
7.Okimoto S, et al. Association of viral isolates from stool samples with intussusception in children. Int J Infect Dis. 2011 Sep. 15(9):e641-5. [Medline].
8.Congenital diaphragmatic hernia. Semin Pediatr Surg. 2010 Aug 19(3):180-5. doi: 10.1053/j.sempedsurg.2010.03.001.
9.Neville HL, et al; Bilateral congenital diaphragmatic hernia. J Pediatr Surg. 2003 Mar 38(3):522-4.
10.van den Hout L, et al; Can we improve outcome of congenital diaphragmatic hernia? Pediatr Surg Int. 2009 Sep 25(9):733-43.
11.Banac S et al. Congenital diaphragmatic hernia in older children Acta Med Croatica. 2004;58(3):225-8.
12.de Goede B, Verhelst J, van Kempen BJ, Baartmans MG, Langeveld HR, Halm JA, et al. Very low birth weight is an independent risk factor for emergency surgery in premature infants with inguinal hernia. J Am Coll Surg. 2015 Mar. 220 (3):347-52. [Medline].
13.Rutherford RB, et al. Meckel’s diverticulum: a review of 148 pediatric patients with special reference to the pattern of bleeding and to mesodiverticular bands. Surgery 1966;59:18-26.
2017.7.26
COPYRIGHT © SEICHOKAI YUJINKAI. ALL RIGHTS RESERVED.